This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Read More
Customize Consent Preferences
We use cookies to help you navigate efficiently and perform certain functions. You will find detailed information about all cookies under each consent category below.
The cookies that are categorized as "Necessary" are stored on your browser as they are essential for enabling the basic functionalities of the site. ...
Always Active
Necessary cookies are required to enable the basic features of this site, such as providing secure log-in or adjusting your consent preferences. These cookies do not store any personally identifiable data.
Functional cookies help perform certain functionalities like sharing the content of the website on social media platforms, collecting feedback, and other third-party features.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics such as the number of visitors, bounce rate, traffic source, etc.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Advertisement cookies are used to provide visitors with customized advertisements based on the pages you visited previously and to analyze the effectiveness of the ad campaigns.
Vaccines provide incredible value in more ways than one. In addition to saving the lives of millions of children, vaccine programs also provide a high economic return on investment. New research demonstrates the incredible impact and value of vaccination for policymakers.
Key Messages
The COVID-19 pandemic has disrupted routine immunization services across the globe. Maintaining pre-pandemic progress in routine immunization programs can save millions of lives and billions of dollars.
Every US $1 invested in vaccine programs returned an estimated $20 in saved healthcare costs, lost wages, and lost productivity, according to new research from the Decade of Vaccine Economics (DoVE) Project.
Using a Value of a Statistical Life approach to model the value of immunization, vaccine programs returned an estimated US $52 for every $1 invested.
Between 2020 – 2030, vaccination programs against 10 pathogens in 98 countries are projected to save 32 million lives, the vast majority (28 million) will be children under 5 years old.
Sustaining Pre-Pandemic Immunization Projected to Save Millions of Lives
A comprehensive study of the impact of vaccination programs, published in The Lancet, estimates that vaccine programs targeting 10 diseases will have saved 69 million lives in 98 low- and middle-income countries (LMICs) between 2000 and 2030. With the COVID-19 pandemic disrupting routine immunization programs across the globe, this research highlights “what might be lost if current vaccination programs are not sustained.” This new analysis provides important evidence demonstrating the value of sustained investment in vaccination coverage, particularly in LMICs.
“In a time when the world desperately awaits a COVID-19 vaccine to help return our lives to normal, this study demonstrates how vaccines have transformed the health of the world, and given 36 million children another chance at life,” said lead study author, Dr. Xiang Li.
The 10 vaccine-preventable diseases included in the analysis were: hepatitis B, Haemophilus influenzae type b (Hib), human papillomavirus (HPV), Japanese encephalitis, measles, meningitis A (Neisseria meningitidis serogroup A), pneumococcal disease (Streptococcus pneumoniae), rotavirus, rubella, and yellow fever.
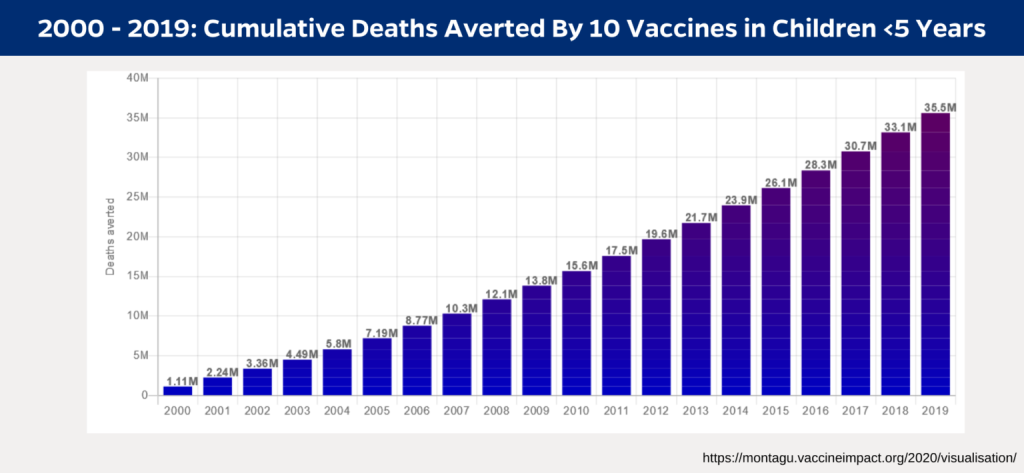
Key Findings: Lives Saved 2000 – 2019
From 2000 through 2019, these 10 vaccines have saved 37 million lives across 98 countries. The vast majority of deaths prevented by these vaccines – 36 million – were children younger than 5 years old.
Between 2000 and 2019 vaccination against these 10 common infectious diseases reduced deaths in children under 5 by nearly half (45%). That is, in the absence of vaccination, all-cause mortality among children younger than 5 years would be 45% higher than currently observed.
Across 73 Gavi countries, 35 million deaths were averted between 2000 and 2019.
Of the ten pathogens included in the analysis, vaccination against measles had the largest impact, with 33 million estimated deaths averted between 2000 – 2019: The equivalent to over 1.6 million deaths averted every year. The analysis projects that vaccination against measles will continue to save even more lives in the next decade (2020 – 2030) with an average of over 2.1 million deaths averted per year.
This tool shows the Vaccine Impact Modelling Consortium’s estimates of health impact from vaccination against 10 pathogens in 98 low and middle income countries from 2000 to 2019. Check out https://montagu.vaccineimpact.org/2020/visualisation/ to create your own visualizations.
Maintaining Progress: Saving Lives in the Next Decade
Maintaining progress on immunization is essential to preventing millions of unnecessary deaths over the next 10 years, particularly in children under 5. The Lancet study, conducted by the Vaccine Impact Modelling Consortium, predicts that if pre-pandemic immunization progress is sustained over the next decade (2020 – 2030) that vaccines will continue to play a vital role in protecting children across the world, particularly those living in the world’s poorest communities.
From 2020 – 2030, these 10 vaccines are projected to save 32 million lives across all ages and 28 million children under age 5.
“A child born in 2019 will experience a massive reduction in their risk of dying from these 10 pathogens over their lifetime, with their mortality falling by 72% due to vaccination alone,” explained study author Dr. Katy Gaythorpe.
The study also calculated disability-adjusted life years (DALYs) averted by vaccination. One DALY represents the loss of the equivalent of one year of full health. The study estimates that in the next decade (2020 – 2030) vaccines will avert 2.1 billion DALYs across all ages and 1.8 billion DALYs in children younger than 5 years old.
The Economic Benefits of Vaccine Programs far Outweigh Their Costs
Preventing illness through vaccination doesn’t just save lives, it also keeps people out of poverty and provides countries with a high economic return on investment. When children get sick, parents can be burdened with crippling financial costs. These costs can include medical care, transportation for treatment, and lost wages.
Investing in immunization programs in the world’s poorest countries yields a significant return on the initial investment. New research from the Decade of Vaccine Economics (DoVE) project, published in Health Affairs, measured the impact of immunization programs against ten pathogens (Haemophilus influenzae type b, hepatitis B, human papillomavirus, Japanese encephalitis, measles, Neisseria meningitidis serotype A, Streptococcus pneumoniae, rotavirus, rubella, and yellow fever) in 94 low- and middle-income countries from 2011 through 2030.
Understanding the DoVE Approach
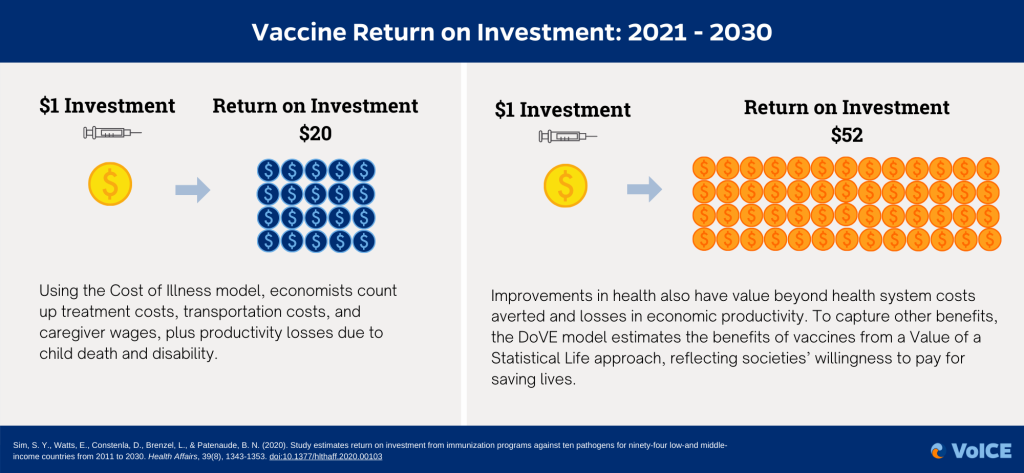
This new DoVE study modeled the return on investment of immunization programs by using two analytical modeling approaches to capture different aspects of the economic benefits of immunization.
The Cost of Illness approach captures the observable impact of immunization programs on household costs, health care costs, and labor productivity.
The Value of a Statistical Life approach reflects the less tangible costs associated with societies’ willingness to pay for saving lives.
Key Findings: Vaccines are a Smart Investment
The economic benefits of vaccine programs far outweigh their costs. With an investment of just a few dollars per child, vaccination can prevent life-threatening illnesses, life-long disability, and medical impoverishment for families.
The analysis estimates that from 2011 to 2030 vaccine programs will generate a net benefit of billions of dollars in savings across countries: $1,445.3 billion using the Cost of Illness modeling approach and $3,371.5 billion with the Value of a Statistical Life approach.
From 2021 to 2030, every US $1 invested in vaccine programs averted around $20 in healthcare costs, lost caregiver wages and missed work, and lost productivity.
Assessing return on investment based on the value societies place on saving lives (a Value of a Statistical Life approach), vaccine programs returned about US $52 for every $1 spent from 2021 to 2030.
For comparison, publicly traded American companies in the S&P 500 have returned an average of US $2.16 for every $1 invested after ten years.
Across all countries and years included in the analysis, vaccination against measles accounted for the majority of economic benefits (76.4% using the Cost of Illness modeling approach and 58.5% using the Value of a Statistical Life approach modeling approach) generated by vaccine programs.
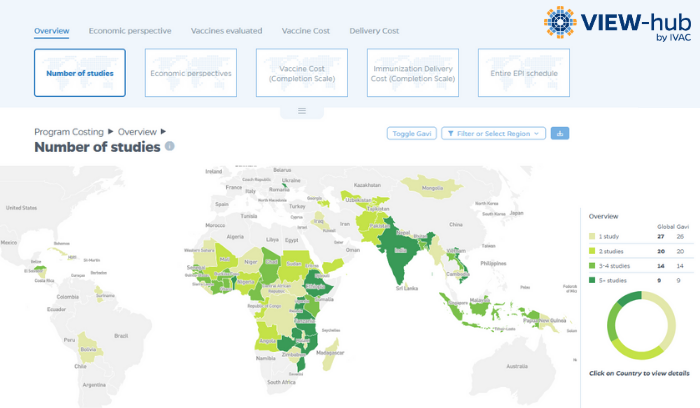
Visualizing Immunization Program Costing and Economic Burden
VIEW-hub, a map-based platform for visualizing data on vaccine use and impact, recently released a new interactive module on immunization economics.
The new module displays cost-of-illness and program costing information from recent DoVE publications in interactive maps and informative country profiles.
The story of immunization is often headlined with the remarkable health benefits—millions of lives saved, and illnesses and hospitalizations prevented. But the true impact of vaccination is even more far-reaching, touching many areas of people’s lives from supporting early childhood growth and development to improving educational outcomes and productivity, promoting economic stability, and helping to address equity gaps: It’s seemingly impossible to undersell the importance of vaccination.
This World Immunization Week, the VoICE editors highlight some of the broader benefits of immunization—not only helping to prevent illness and save lives, but also promoting healthy development, productivity, economic stability, and equity for all.
Key Messages
Only looking at the direct impact of vaccination on morbidity and mortality grossly underestimates the wider value of vaccination on overall health and development
Several studies show that immunization has the potential to increase productivity by averting preventable illness
Vaccines are associated with improved cognitive ability, education, and healthy physical development – which translates into increased economic productivity
Vaccine-preventable diseases disproportionately affect the poorest children and families, but immunization can be a cost-effective tool to improve equity across geographies, gender, and marginalized populations
Preventing Pandemics Supports Economic Stability
The global health community is now facing an unprecedented challenge in the COVID-19 pandemic. As countries across the world attempt to slow the virus’s spread, this event has become a potent reminder of the vital importance of vaccination; we are seeing today just how much an infectious disease outbreak can ravage both national and global economies. Vaccines are important tools to help avert potentially catastrophic health costs that arise from preventable infectious disease outbreaks. Several studies have found that vaccines can bring additional stability to national economies by preventing the high costs incurred by illnesses.
A 2009 study in Africa found an economic loss of US $43-72 million resulting from the 110,837 cases of cholera reported in 20071.
Researchers modeling the costs of potential pandemic influenza in the UK estimated costs of illness between £8.4 and £72.3 billion depending on the severity of the fatality rate, and even larger still for an extreme pandemic. In such a scenario, vaccination could limit the overall economic impact of pandemics2.
Vaccines Help Promote Productivity
Productivity—the measure of output by a working individual or a population—is an important determinant of standard of living. By preventing illness, vaccination can help promote productivity by supporting healthy cognitive development and success in school, ultimately helping children achieve their full potential across the lifespan.
A 2019 longitudinal study followed almost 6,000 children in India, Ethiopia, and Vietnam throughout childhood, finding that those vaccinated against measles scored better on cognitive tests of language development, math, and reading compared to children who did not receive measles vaccines3.
In a 2011 study in the Philippines, children vaccinated against six diseases performed significantly better on verbal reasoning, math and language tests than unvaccinated children4.
Vaccine-preventable diseases lead to both work and school absenteeism, which can negatively impact productivity and cause a substantial economic burden. A Norwegian study found that children hospitalized with rotavirus were absent from daycare for 6.3 days, on average, and 73% of their parents missed work5.
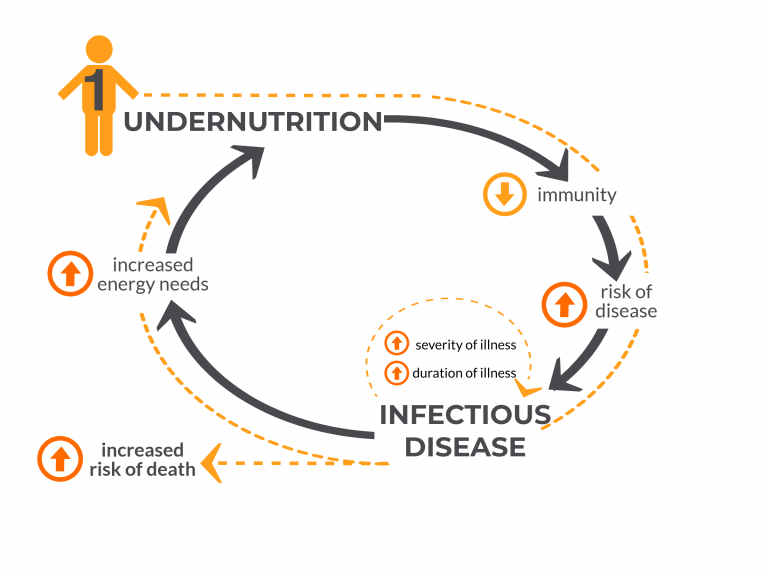
Vaccines Support Healthy Child Growth and Development
Some vaccine-preventable diseases can delay or interrupt normal growth and development in early childhood, leading to long-lasting damage that can adversely impact children for the rest of their lives. Persistent or recurrent infections in early life can lead to poor growth and stunting, which in turn can adversely affect adult health, cognitive capacity, and economic productivity.
Childhood vaccination programs can be a tool for mitigating undernutrition in developing countries. Children enrolled in Universal Immunization Programs observe improvements in terms of age-appropriate height and weight as per results of a study focused on 4-year-old children in India. On average, height and weight deficits were reduced by 22-25% and 15% respectively6.
A study in Kenya revealed that polio, BCG, DPT and measles immunization had protective effects with respect to stunting in children. In children under the age of 2 years, children immunized with polio, BCG, DPT, and measles vaccines were 27% less likely to experience stunting compared to unimmunized children7.
A 2013 study conducted in several developing countries found that children with moderate-to-severe diarrhea grew significantly less in length in the two months following an episode of illness compared to age- and gender-matched controls8.
Modeling of data from India’s 2005-2006 National Family Health Survey indicated that vaccinations against DPT, polio, and measles were significant positive predictors of a child’s height, weight, and hemoglobin concentration. Such indicators, in turn, influence children’s cognitive development and hence the future supply of skilled labor that is critical for economic growth9.
Tackling Immunization Inequities Can Have Substantial Benefits
While huge progress has been made in introducing and scaling up access to important vaccines, we still have a long way to go. There is significant evidence of inequities in vaccine coverage that exists between and within countries, as well as between and within different populations. In Gavi-supported countries, there are still an estimated 10.4 million “zero-dose children” who have not received any doses of DTP-containing vaccine.
Results of a 2019 study in Kenya found that immunization outreach for remote or hard-to-reach populations can still be highly cost-effective. The study found that failure to vaccinate hard-to-reach children against measles would result in more than 1,400 measles cases, 257 deaths, and cost nearly U.S. $10 million over the course of 4 years, mainly due to productivity losses from caretakers missing work10.
A 2018 study found that children of poor labor migrants living in Delhi, India are much less likely to be fully vaccinated than the general population and thus are at greater risk of vaccine-preventable diseases. Only 31% – 53% of children from migrant families were fully immunized (against 7 diseases) by 12 months of age, compared to 72% in the overall population of Delhi — with recent migrants having the lowest rates11.
Researchers looking at vaccination coverage in 45 low- and middle-income countries found that maternal education is a strong predictor of vaccine coverage. Children of the least educated mothers are 55% less likely to have received measles-containing vaccine and three doses of DTP vaccine than children of the most educated mothers12.
The evidence shows that vaccines offer cross-cutting benefits for individuals, families, communities, and truly everyone across the globe. Cross-disciplinary research from many global health perspectives demonstrates that vaccines as a versatile, impactful tool that does so much more than just preventing millions of deaths and illness every year: Vaccines benefit global economies, boost productivity, and help close gaps in equity.
As we respond to COVID-19, the reality that infectious disease outbreaks anywhere in the world can quickly become a threat anywhere further highlights the importance of investment in vaccination as a part of strong, resilient health systems. As countries across the world grapple with containing the COVID-19 outbreak, we must also work together to ensure that the world’s most vulnerable children don’t miss out on the vaccines that prevent devastating illnesses like measles, polio, diarrhea, and pneumonia. In the face of this current challenge, it’s essential that we work together to protect essential health services like immunization to ensure that all people have a shot at living a healthy life protected from preventable disease.
Kirigia, J.M., Gambo, L.G., Yolouide, A., et al 2009. Economic burden of cholera in the WHO African Region. BMC International Health and Human Rights. 9(8). doi: 10.1186/1472-698X-9-8
Smith, R.D., Keogh-Brown, M.R., Barnett, T., et al 2009. The economy-wide impact of pandemic influenza on the UK: a computable general equilibrium modeling experiment. BMJ. 339. https://doi.org/10.1136/bmj.b4571
Nandi A, Shet A, Behrman JR, et al. 2019. Anthropometric, cognitive, and schooling benefits of measles vaccination: Longitudinal cohort analysis in Ethiopia, India, and Vietnam. Vaccine. 37. https://doi.org/10.1016/j.vaccine.2019.06.025
Bloom, D. E., Canning, D., & Shenoy, E. S. (2011). The effect of vaccination on children’s physical and cognitive development in the Philippines. Applied Economics, 44(21), 2777-2783. https://doi.org/10.1080/00036846.2011.566203
Edwards CH, Bekkewold T, Flem E. 2017. Lost workdays and healthcare use before and after hospital visits due to rotavirus and other gastroenteritis among young children in Norway. Vaccine. 35. https://doi.org/10.1016/j.vaccine.2017.05.037
Anekwe, T.D., Kumar, S. 2012. The effect of a vaccination program on child anthropometry: Evidence from India’s Universal Immunization Program. Journal of Public Health. 34(4). https://doi.org/10.1093/pubmed/fds032
Gewa, C.A. and Yandell, N. 2011. Undernutrition among Kenyan children: contribution of child, maternal and household factors. Public Health Nutrition. 15(6). https://doi.org/10.1017/S136898001100245X
Kotloff, K.L., Nataro, J.P., Blackwelder, W.C., et al 2013. Burden and aetiology of diarrhoeal disease in infants and young children in developing countries (the Global Enteric Multicenter Study, GEMS): a prospective, case-control study. Lancet. 382(9888). https://doi.org/10.1016/S0140-6736(13)60844-2
Bhargava, A., Guntupalli, A.M., Lokshin, M. 2011. Health Care Utilization, socioeconomic factors and child health in India. Journal of Biosocial Sciences. 43(6). https://doi.org/10.1017/S0021932011000241
Lee BY, Brown ST, Haidari LA et al. 2019. Economic value of vaccinating geographically hard-to-reach populations with measles vaccine: a modeling application in Kenya. Vaccine. 37(17). https://doi.org/10.1016/j.vaccine.2019.03.007
Kusuma YS, Kaushal S, Sundari AB, et al. 2018. Access to childhood immunization services and its determinants among recent and settled migrants in Delhi, India. Public Health. 158. https://doi.org/10.1016/j.puhe.2018.03.006
Arsenault, C., Harper, S., Nandi, A., et al. 2017. Monitoring equity in vaccination coverage: A systematic analysis of demographic and health surveys from 45 Gavi-supported countries. Vaccine. 5(6). https://doi.org/10.1016/j.vaccine.2016.12.041
World Immunization Week 2020 (April 24-30) is an opportunity for immunization advocates across the world to promote the value of vaccines for protecting people of all ages against preventable diseases. Our VoICE social media toolkit provides messaging on the vital role that vaccines play in global health. Beyond saving millions of lives every year #VaccinesWork For All by strengthening our health care systems, protecting global health security, shrinking equity gaps, and more.
Join us in promoting the message that #VaccinesWork For All by sharing the evidence on the broad benefits of immunization!
VoICE Social Media Toolkit for World Immunization Week 2020
Download the VoICE World Immunization Week 2020 Toolkit for a series of social media messages and shareable images that highlight key evidence on the value of vaccines! Messaging covers the six main topics of the VoICE Compendium: Health, Education, Economics, Equity, Health Systems and Integration, and Global Issues.
The toolkit is also available as a downloadable PDF and all images can be easily copied or saved directly from this page.
Welcome to WIW 2020!
Immunization saves millions of lives every year. Yet, there are still nearly 20 million children worldwide who are not getting the vaccines they need.
We have it in our power to close this gap!
#VACCINESWORK TO PROTECT OUR HEALTH
#DYK those with HIV, cancer, and weakened immune systems benefit from immunization of others through herd immunity?
#VaccinesWork for all by protecting people around us, especially those who are vulnerable like new babies, older adults, and people who are seriously ill.
#DYK that immunization is linked to improved education and cognitive outcomes? Immunized children stay healthier so they miss less school and attain higher school grades.
Vaccines don’t just save lives; they keep the world’s most vulnerable people out of poverty. A 2018 @Health_Affairs study found the poorest households receive the most benefit from increased access to vaccines.
13.5 million children around the world still can’t access vaccines – these children are often the most vulnerable to disease and health disparities. We have it in our power to close this gap!
Leaving no child behind means ensuring the most marginalized – those touched by conflict or forced from their homes – have access to lifesaving #vaccines.
In Kenya, rates of pneumonia hospitalizations in children <5 dropped by 27% after 4 years of PCV10. #VaccinesWork for All to reduce hospital admissions and free up more resources to treat and prevent other illnesses.
Between 2005-2014 nearly 400 infectious disease outbreaks (excluding measles) were reported to the @WHO, threatening the health security of the entire world.
2019 saw a record for measles outbreaks – more than 140,000 lives were lost, mostly children.
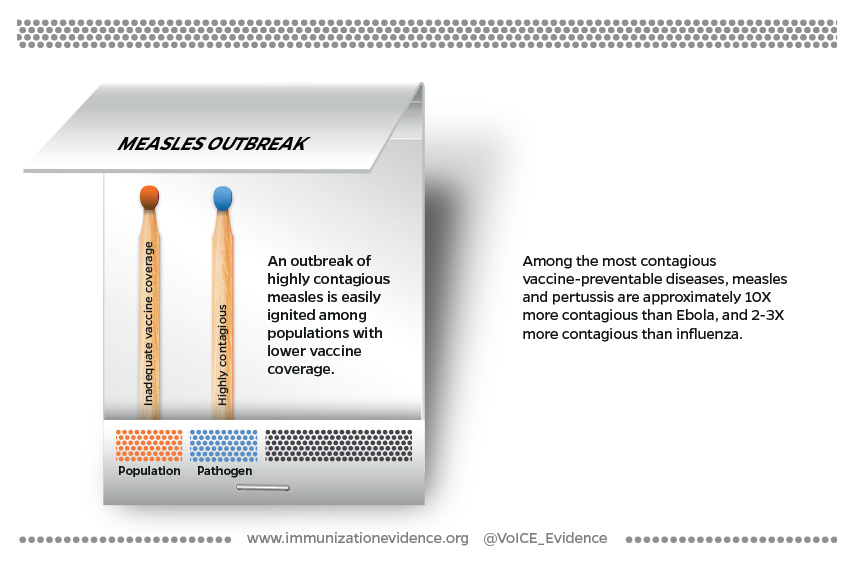
Measles is so contagious that the exposure of a single person without immunity to the virus can spark an outbreak that quickly burns through whole communities.
From Abuja to Atlanta, recent infectious disease outbreaks have all too commonly captured the regular news headlines. In this Featured Issue on vaccine-preventable disease outbreaks, the VoICE team goes past the headline, down to the fine print. We bring you an evidence-backed overview of vaccine-preventable infectious disease outbreaks worldwide, with a special focus on the circumstances that increase the likelihood of an outbreak, the less-obvious health and economic consequences, and a “top five” list for outbreak prevention and preparedness.
Infectious disease outbreaks can happen anywhere and have significant, and often hidden, social, health and economic repercussions.
A large proportion of recent infectious disease outbreaks are of vaccine-preventable diseases.
The likelihood or severity of an outbreak is increased by factors such as low vaccination coverage, crowding, poor sanitation, malnutrition, and human mobility.
Outbreak prevention and preparedness needs to be systematically integrated into health systems and specific areas must urgently be strengthened to include immunized healthcare workers, streamlined health communications, and ready surveillance systems.
There are a triad of elements that influence the likelihood and severity of an infectious disease outbreak. These include factors related to:
The Pathogen – aspects of the disease agent itself (virus or bacteria), such as how it is transmitted from person to person, how contagious it is, the incubation period before symptoms appear, how severe the infection may be and how likely it is to result in death.
The Population – factors affecting the state of health of the population at risk, including the proportion vaccinated, malnourished or living in sub-optimal conditions such as overcrowding, and how people move on small or large spatial scales.
The Environment – generally refers to environmental factors that affect the spread of disease such as access to clean water and sanitation, access to health care, social norms and cultural practices – for example in the case of Ebola where traditional burial practices bring people into contact with infected bodily fluids which transmit the virus.
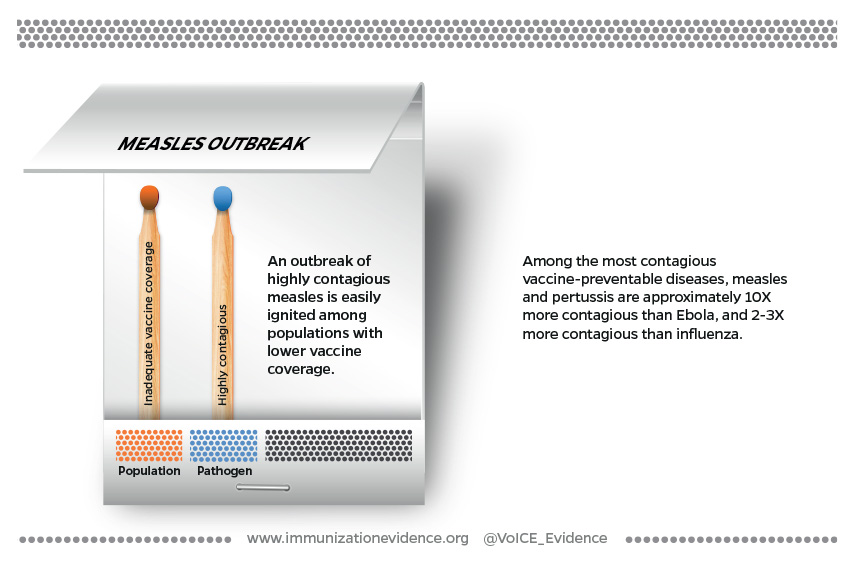
Figure 1: Pathogen, population, and environmental factors can ignite an outbreak of infectious disease.
An outbreak can ignite when sparked by only a handful of the factors described above, such as in the case of measles or pertussis – two highly contagious pathogens which can rapidly take advantage of gaps in vaccine coverage. In other circumstances, parts of all three elements – pathogen, population and environment – are present and create the perfect conditions to kindle an outbreak.
Cracks in the immunization firewall
A high firewall of immunization coverage with very very few gaps is required to protect populations from outbreaks of highly transmissible and contagious infections, such as measles or pertussis, which have the potential to spread rapidly and far. An infection like measles is so contagious that almost all susceptible people who are exposed will become infected meaning that about 95% of a community needs to be protected to stop measles virus transmission. Add to that the fact that contagiousness occurs before the telltale rash (and very often before anyone knows what is causing the illness), and you can see how just those two pathogen-related factors cause some outbreaks to explode. In a community with lower than 95% vaccine coverage, the exposure of a single person without immunity to the virus is the single spark that is needed to start an outbreak that quickly burns through a community of people who have little or no immunity. The connection between measles and low vaccination coverage is so strong that some researchers describe measles outbreaks as being a “canary in a coalmine” that brings to light programmatic weaknesses in immunization coverage in places where data on vaccination coverage is thin or unreliable.
Figure 2: Factors contributing to measles outbreaks.
The firewall for a disease like Ebola must be just as strong but for different reasons. Ebola is not very contagious when compared to other infections, but has an exceedingly high risk of death – up to 70% with some strains. (An animated visualization from the Washington Post of the relative contagiousness and mortality risk of different diseases.) When and exactly where the disease will appear is impossible to predict (see “The case of Ebola, a zoonotic infection”, below) and a vaccine against the disease has not yet been approved. For these reasons, outbreak control measures for Ebola, including significant efforts to find people who have been exposed, must be swift and widespread. An experimental vaccine for Ebola is being used in a “ring” vaccination strategy to vaccinate everyone who has come in contact with someone who has the disease, and has proven to be nearly 100% effective in preventing infection, if administered soon enough after exposure. Gaps in this vaccination ring mean the deadly disease has the potential to continue spreading.
Complex emergencies
Global socio-political events, including armed conflicts and other complex humanitarian emergencies, can result in a highly flammable set of circumstances – a “box of matches” containing nearly every population and environmental factor, which can easily spark a significant outbreak. In a study of the overlap between complex humanitarian emergencies and disease outbreaks, researchers found that more than 40% of complex emergencies that occurred between 2005-2014 were associated with an outbreak of infectious disease, with a high likelihood that the outbreak was vaccine-preventable.
The mass migration of people that often results from complex humanitarian emergencies can set off a “risk factor cascade”, that includes decreasing vaccination coverage, undernourishment, overcrowding, and poor sanitation, dramatically increasing the risk of an outbreak with each added cascade factor.
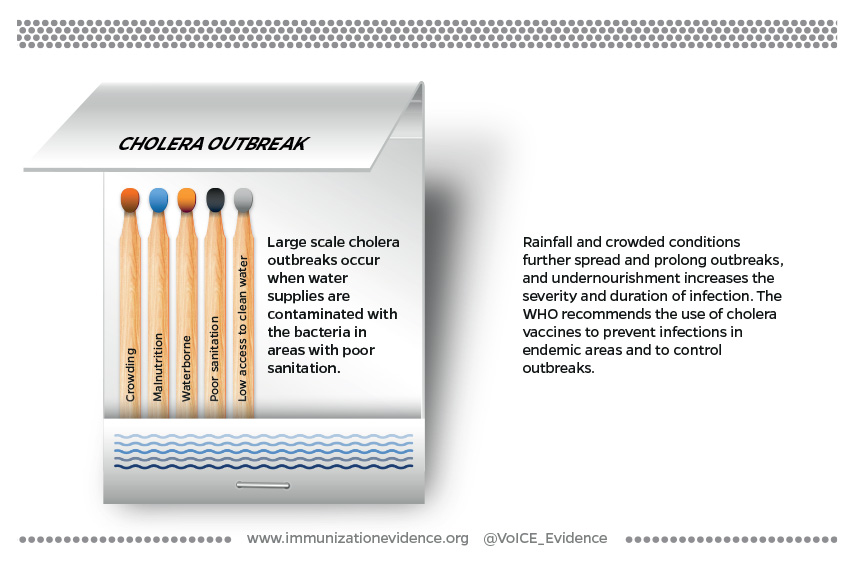
When environmental conditions are poor and pathogen-related factors are significant, only a tiny spark is required to ignite an outbreak, as is often the case with cholera. The bacteria that causes cholera (Vibrio cholera), a highly contagious diarrheal disease, can be quickly passed to large numbers of people through contaminated water in crowded and poorly-resourced settings such as urban slums or refugee camps that have poor access to clean water and sanitation. Rainfall further spreads the contaminated water, sustaining the outbreak. Population factors, such as undernutrition further worsen the disease. Undernourished people are at greater risk of severe cholera infections and of dying from the infection.
Figure 3: Factors contributing to cholera outbreaks.
The case of Ebola, a zoonotic infection
Most vaccine-preventable outbreaks are due to pathogens which circulate constantly among humans, causing spikes in disease when population and environmental conditions allow. Ebola, however, is a zoonotic infection, meaning that the normal reservoir for the pathogen is among animals, most likely bats. Ebola outbreaks among humans are triggered when people come into contact with infected animals (such as through the consumption of bush meat from infected primates), become ill and then pass the virus to other humans where it spreads until it can be contained.
Predicting when and where the virus will strike and spark an outbreak is thus very difficult, which significantly adds to the challenges of planning for, controlling and mitigating the impact of outbreaks. Ebola is one of several diseases of zoonotic origins that has the potential to ignite a global pandemic, according to USAID.
The Repercussions of Vaccine-Preventable Outbreaks
While outbreaks of measles and Ebola have been widely covered in the news media, a less visible topic has been the significant – and sometimes long-term – health and economic repercussions that come along with outbreaks of these and other diseases.
Repercussions on health systems
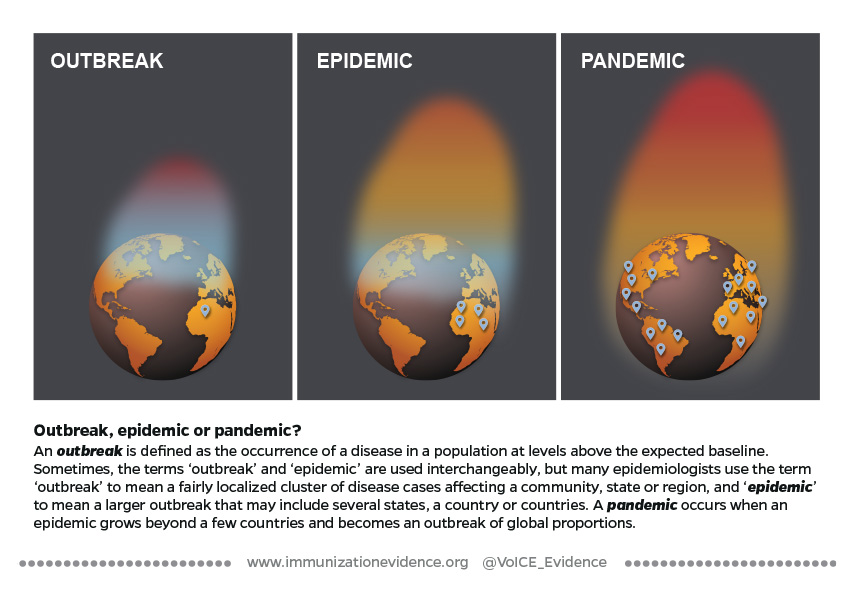
By definition, an outbreak is the occurrence of disease in a population that rises above expected levels. Although contingency plans may be in place for dealing with an outbreak, health staff, funding, medical supplies and other resources are often diverted to outbreak control, weakening the provision of other health services. In one example from Burkina Faso in 2007, meningitis epidemics disrupted health services at every level. Impact on all people seeking healthcare included longer wait times to be seen, increased time for lab test results, higher stress among caregivers and an increase in the number of misdiagnoses by overtaxed health care workers (HCWs).
Repercussions for healthcare workers
The burden on HCWs, in fact, extends beyond exhaustion and the mental toll of working in outbreak conditions. Health workers themselves are at significant risk of becoming victims of an infectious disease outbreak and passing on the infection to others, in particular before the infectious agent has been identified. HCWs can account for a substantial proportion of disease cases. A recent study using data from historical outbreaks of Ebola in Guinea and Nigeria, found that (had a fully effective vaccine been available at the time of those outbreaks) prophylactically vaccinating healthcare workers would have decreased the size of the Ebola epidemics in those countries by 60-80%. In the US, researchers estimated that ensuring full vaccination of healthcare workers would prevent more than 45% of exposures to pertussis that occur in healthcare settings. These are only two of many examples illustrating the disproportionate burden of disease cases among HCWs, all of which highlight critical gaps in vaccine coverage among people at significantly increased personal risk, and risk of infecting others. (For more on the WHO’s recommendations for immunizing health care workers.)
Repercussions of every kind: The Ebola firestorm
Outbreaks of exceptionally deadly infectious diseases such as Ebola can cause a cascade of events affecting every person and sector in a community and thus represent a firestorm of all the potential repercussions of an outbreak occurring at once. Huber et al described the devastating and far-reaching impact of the 2014 Ebola outbreak in West Africa, including more than half a million people experiencing food insecurity, school closures lasting more than 7 months, tens of thousands of children orphaned, a huge proportion of the health workforce killed by the disease, infant, maternal and child deaths from lack of skilled health workforce and a 97% reduction in surgical capacity, to name a few. A second study projected that the crippling of immunization programs resulting from the Ebola outbreak could double the number of people at risk for measles, ultimately killing nearly as many people as Ebola itself.
At ALIMA’s (The Alliance for International Medical Action) Ebola Treatment Center in Beni, Democratic Republic of the Congo’s North Kivu Province, health workers care for patients infected with Ebola within ALIMA’s innovative biosecure emergency care unit – the CUBE.
Economic repercussions: costs of outbreaks
Adding to the secondary health and societal costs of infectious disease outbreaks are the actual monetary and economic impacts, which are significant even in a relatively small and quickly contained outbreak. The larger and longer an outbreak, the more significant its macroeconomic impacts on productivity, import & export losses, reduced tourism revenue and consumption.
From cholera to measles to Ebola, health economists have published several studies on the economic impact of outbreaks, covering direct costs of outbreak management to slowed national economic growth as a result of outbreaks. Direct costs to health systems include outbreak investigation costs such as personnel, supplies, travel expenses to find people exposed to infection and outbreak containment efforts including vaccination or prophylactic treatment costs for those exposed. Costs to individual families seeking treatment can be significant and have long-term economic consequences. Productivity losses and reduced consumption and revenue directly affect nations dealing with outbreaks, but shifts in imports and exports internationally can impact other nations economically, despite not being directly affected by the outbreak. Just some of the economic repercussions can be found in the cases below:
A measles outbreak of 3 cases in Iowa, USA in 2004 cost the state Department of Public Health more than $140,000 in direct costs over a 2-month period to contain and manage the outbreak.
A 2014 measles outbreak in Micronesia cost approximately US$4 million in direct costs, lost caretaker productivity and significant outbreak containment expenses. This amount is equal to the entire annual budget for education in the small island nation.
A study of the economic burden of cholera in Africa found that 110,000 the cases of cholera reported in 2007 alone resulted in economic losses to the continent of $43.3 million, $60 million and $72.7 million US dollars, assuming life expectancies of 40, 53 and 73 years respectively.
A study of a cholera outbreak in Peru in 1991-92 estimates that the national economy conservatively suffered more than US$50 million in economic losses due to reduced tourism revenue, reduced revenue on export of goods and lower domestic consumption as a result of the outbreak of cholera.
In a comprehensive accounting of the costs of the 2014 Ebola outbreak in West Africa, Huber et al estimate the economic and social costs to have been US$53 billion, of which US$18.8 billion was attributed to non-Ebola deaths.
Outbreak Prevention and Preparedness
The prevention, mitigation and control of infectious disease outbreaks is becoming more urgent, while the number of emerging diseases increases, populations are more mobile and economies are stretched thin. Addressing infectious disease outbreaks must be a high political priority, requiring investments of both financial support and political will. But investments inwhat exactly?
It will come as no surprise that vaccination features prominently in our “TOP FIVE” list of investments that must be made to better prevent and prepare for outbreaks of infectious disease. What may be surprising is that financing, purchasing and delivering vaccines to the general population is only one of the necessary steps towards ensuring that the full potential of immunization can be realized in helping to prevent, mitigate and control outbreaks. Clear and actionable preparedness plans, robust health systems with increased access to health care, and significantly increased investments in disease surveillance and health communication round out our list.
Top Five Investments In Outbreak Prevention And Preparedness
1. Investment in health systems, including routine immunization
A country’s ability to prevent, detect and respond to outbreaks is tied to the strength and capacities of its health system overall. As such, a 2018 multi-stakeholder outbreak preparedness framework includes strengthening overall public health system capacity as the first of four pillars in the prevention of significant disease epidemics and pandemics.
National and subnational health systems supported by recommended levels of funding, high political priority and strategic planning processes that include the integration of emergency preparedness and everyday health systems operations are more resilient to emergencies such as disease outbreaks, and can recover more quickly. A 2016 WHO-led consultation with countries in the African region found that health systems and health security-related structures functioned independently from one another, but that strong support existed for the integration of emergency prevention and preparedness in broader health systems.
Given the high proportion of outbreaks due to vaccine-preventable infectious diseases, immunization has an especially important role to play in the prevention of disease outbreaks, and is thus critical for emergency prevention and preparedness.
2. Full immunization for health workers
High coverage of routine immunization is a critical firewall to prevent outbreaks from occurring, and vaccination of healthcare workers is especially critical to minimizing the spread of an emerging outbreak. Several studies have demonstrated the significant return on investment to be had by ensuring HCWs are fully immunized, given that HCWs often account for a disproportionately large number of disease cases. In the US study looking at prevention of the spread of pertussis referenced above, the financial return on vaccinating healthcare workers in hospitals was estimated to be nearly two and a half times the cost invested. A similar study of pertussis vaccine and HCWs in the Netherlands estimated the return on investment to be four times as great as the initial cost.
3. Actionable preparedness plan
Despite strong evidence that prevention and preparedness provide a sizeable return on investment, compared to the costs of an unchecked outbreak of disease, between 2016 and 2018 only one third of countries had assessed their own capacity to prevent, detect and control disease outbreaks.[1] That number has now risen to just under half, but nearly 80% of countries who have completed a preparedness assessment are wholly or partially unprepared for an outbreak of disease.[1] Experts argue that the cycle of panic and neglect in addressing disease outbreak readiness is a crisis of global proportions, and one which can only be broken by implementing and monitoring concrete preparedness plans.
4. Public health communications
Following recent global disease events like Ebola and SARS, which ignited global panic about the outbreaks and their impact, recognition has been increasing of the importance of consistent, clear and culturally sensitive communication with the public around health issues. Investment of money and time in this area, however, still lags behind the need. The WHO’s Outbreak Communication guidelines emphasize not only what needs to be done to communicate during an outbreak, but also the importance of building and maintaining trust in national and health authorities among all communities as a foundation for health communications and care seeking overall. Trust in an existing foundation of open, clear communication can help immunize against panic and increase compliance with measures intended to control and end outbreaks.
5. Infectious disease surveillance
The importance of disease surveillance, robust enough to detect outbreaks early, cannot be overstated, and yet, it is an area that is often poorly integrated in the broader public health system, and is chronically underfunded. Considered an essential public health capacity, investments in surveillance as it relates to outbreak detection and control are likely to have important benefits for other health priorities and diseases. For example, polio detection systems in the Americas were leveraged to better detect measles and rubella. Likewise, laboratory experience with measles and rubella surveillance led to the early detection and response to the H1N1 influenza virus in Mexico in 2009.
In summary, the specifics of the strategy for implementing each of these actions vary based on the type of outbreak. For example, the current vaccination strategy for Ebola includes finding and vaccinating all people who have come in contact with someone who has the disease (and all of those contacts’ contacts) to form a “ring” of immunity around disease cases. By contrast, measles and pertussis vaccines are recommended for all children worldwide during early childhood. Despite such differences in the specific approach needed, each of these five areas above are critical for mitigating the immediate impact and secondary repercussions of all future outbreaks.
[1] Jonas, Katz, et al. Call for independent monitoring of disease outbreak preparedness. BMJ. 2018;361:k2269 doi: 10.1136/bmj.k2269
Editorial Commentary
“We are witnessing an apparent increase in the magnitude and frequency of outbreaks due to vaccine-preventable diseases, as adroitly described in this VoICE Featured Issue. Such outbreaks are, by definition, preventable and thus a tragedy, resulting in pointless deaths, countless disabilities, loss of productivity, and economic costs. We must do better. We call on policy makers, community leaders, and the global public health community to improve surveillance systems to detect outbreaks as early as possible, improve vaccination coverage to ensure all children are appropriately immunized, and effectively communicate the benefits of vaccination so trust in public health is restored. We will face new infectious disease threats. We must control those diseases for which we already have safe and effective vaccines so we are best prepared to deal with the emerging ones.”
William Moss, MD, MPH Interim Executive Director, International Vaccine Access Center
William Moss, MD, MPH is Interim Executive Director, at the Johns Hopkins Bloomberg School of Public Health’s, International Vaccine Access Center (IVAC), a pediatrician and infectious disease specialist who has dedicated the last three decades to improving the lives of children through better treatment and prevention of infectious disease. Dr. Moss has made significant contributions in many areas, including HIV, malaria, complex humanitarian emergencies and especially measles, for which he is a member of the World Health Organization’s expert Working Group on Measles and Rubella.
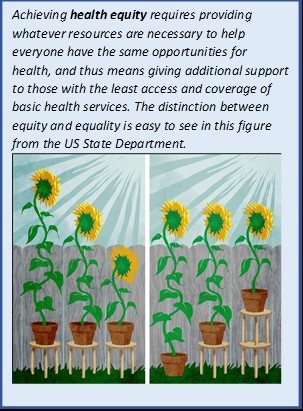
December 12th is worldwide Universal Health Coverage (UHC) day! Although exceedingly complex in its implementation, the concept behind UHC is simple: All people should benefit from quality health services, medicines and vaccinations, and no one should be put in financial peril to do so. In recognition of UHC Day 2018, the VoICE team brings you a brief look at the interplay between coverage of immunization and other basic health interventions, and the important role of immunization in protecting against financial risk – both within the context of the Sustainable Development Goal Target for UHC.
Achieving universal coverage of basic health services will require strengthening and expanding current health systems AND new approaches to reaching those who still cannot or do not access health services.
The reach of immunization delivery programs can be leveraged to provide other basic services – and increase financial efficiency of health systems – and the reverse is also true: the delivery of other interventions can help to increase the uptake of vaccines.
Achievement of UHC will positively contribute to at least six of the 17 Sustainable Development Goals.
Immunization can contribute significantly to achieving financial risk protection against health costs.
Universal Health Coverage and the Sustainable Development Goals
December 12th is worldwide Universal Health Coverage (UHC) day! The aim of drawing attention to this day is to shine the global spotlight on the gaps in achieving health as a human right. Although exceedingly complex in its implementation, the concept behind UHC is simple: All people should benefit from quality health services, medicines and vaccinations, and no one should be put in financial peril to do so.
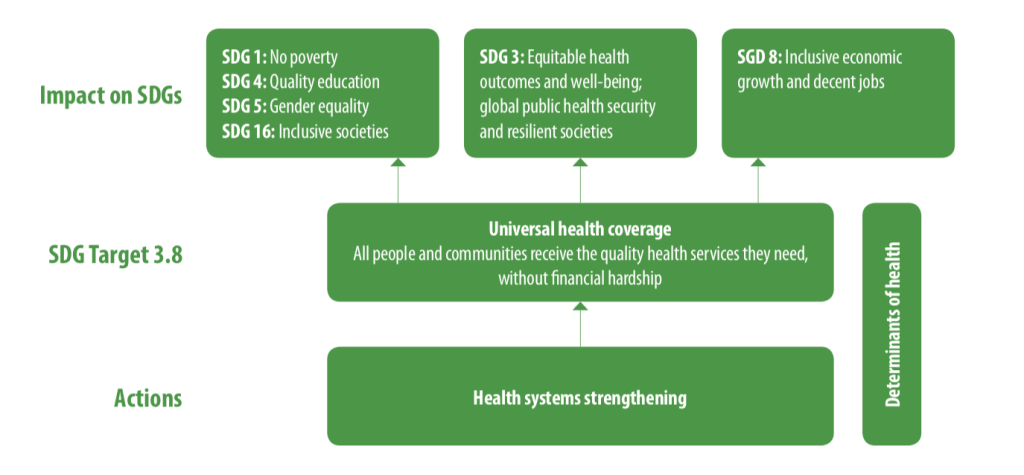
In 2015, 193 United Nations Member States committed to an ambitious set of 17 “Sustainable Development Goals” (SDGs) by 2030. The right to health not only figures prominently as a goal in and of itself – SDG3 is to “Ensure healthy lives and promote well-being for all at all ages” – but is also fundamentally intertwined with goals related to equity, poverty, economic growth and inclusion. (See Figure 1.)
Figure 1: The interrelatedness of Universal Health Coverage with other Sustainable Development Goals, and the importance of health systems strengthening.
Source: Tracking Universal Health Coverage: 2017 Global Monitoring Report.World Health Organization and International Bank for Reconstruction and Development / The World Bank; 2017. License: CC BY-NC-SA 3.0 IGO. Available here: http://www.who.int/healthinfo/universal_health_coverage/report/2017/en/
Embodied in the 8th Target of SDG3 (SDG 3.8), the pursuit of UHC is supported by the twin indicators of 1) coverage of essential services (including immunization), and 2) financial risk protection from the incurrence of economically burdensome health costs. In recognition of UHC Day 2018, the VoICE team brings you a brief look at the interplay between coverage of immunization and other basic health interventions, and the important role of immunization in protecting against financial risk – both within the context of SDG 3.8.
Building on coverage of vaccines gives UHC a head start, but there is more to do
Equity is at the heart of the Sustainable Development Goal target 3.8, which seeks to achieve universal health coverage and financial risk protection for all. The coverage indicator for the achievement of UHC tracks the coverage of 14 “tracer interventions”, which together serve as a barometer for access to basic health services. Access to immunization is tracked through the coverage of the third dose of DTP3, one of four maternal and child health tracer interventions. Although DTP3 coverage is evidence of the fact that immunization is one of the most widely available and equitably distributed interventions worldwide, several other important vaccines lag behind the 85% coverage of DTP3 worldwide in 2017.
Specific vaccines notwithstanding, high coverage with some vaccines such as DTP make immunization programs a critical backbone of any universal health coverage strategy. Routine and campaign-based immunization programs reach some children in remote or poverty stricken areas whose families have little other connection to the health system, and as such, offer opportunities to provide additional basic health care services to children and their families, especially interventions associated with maternal and child health. See Figure 2 for some highlights from VoICE of the opportunities for mutual reinforcement between immunization and other programs.
Figure 2: Examples of the integration of immunization and other health services.
Vitamin A distribution integrated with polio vaccine campaigns led to increased VitA coverage in several African countries.
Delivery of HPV vaccine to school-age girls in Rwanda provided an opportunity to offer school-age boys a variety of health services at the same time.
The timing of childhood immunizations could be harnessed to deliver a range of early childhood development interventions such as newborn hearing screening, sickle cell screening, treatment and surveillance, maternal education around key newborn care issues such as jaundice, and tracking early signs of poor growth and nutrition.
Despite the relatively high coverage globally of some vaccines, other critical vaccines have reached only a small fraction of the world’s children. Fully 15% of the world’s children are not reached at all by immunization – a gap whose distribution carries significant inequity – so vaccine coverage successes are very much tied to the achievement of UHC goals and targets for other health services.
The achievement of UHC targets will, however, require significant reform and expansion of existing health systems to address challenges such as missed opportunities to integrate services. For example, a recent study in 14 low- and middle-income countries found an exceedingly high rate of missed opportunities to vaccinate in 8 of the 14 countries, despite families coming into contact with the health system. For these countries, children failed to be vaccinated more than 50% of the time, despite they or their mother having received at least one of 5 other basic health interventions provided through the health system. Additionally, for the millions of families not reached at all by current health systems, barriers may include socio-cultural factors, in addition to geography, education, poverty, etc.
For these families and others with inadequate health services, a truly equity-driven approach is needed. That is, governments, partners, health-providers, and systems will need find ways to provide whatever additional support is needed to help them catch up, not just make the same resources available to everyone.
For families, financial barriers to immunization are relatively low, but health and economic returns are high
The second indicator of the universal health coverage target acknowledges that the costs associated with health care – both preventative services and treatment for illness – are a significant barrier for hundreds of millions of people around the world. These costs prevent some people from even trying to access health services, and for those who do seek care they cannot afford, the financial burden of these services can have significant, negative and lasting economic impact. The provision of a basic package of preventative services, including immunization, would thus create a positive, reinforcing cycle of increased health-seeking behavior and improved financial stability for individuals, families and economies.
Immunization is a critical element to success for two reasons. First, thanks to global institutions such as Gavi and UNICEF, immunization is free of charge for a large proportion of families in the world’s middle and low-income nations and financial barriers to access are thus relatively low. However, not all crucial vaccines are yet available through national immunization programs in every country. In some places, lifesaving vaccines against disease such as pneumococcal disease are only available through the private market, carrying a price tag far too high for many families to access. And, as mentioned above, sociocultural factors and other issues are significant drivers of gaps in vaccine coverage and these must be addressed carefully and concertedly.
The second reason immunization is critical to meeting the financial risk protection targets of UHC is much more obvious: the widespread use of vaccines has the power to avert significant costs associated with treatment of infections. The huge economic burden of these infections stems from the costs associated with treating relatively low-cost but frequently occurring infections and complicated infections such as meningitis which are rare but very expensive to treat. These vaccine-preventable episodes of illness are responsible for a large number of families being pushed into poverty each year.
The hurdles that remain are high, but health for all awaits on the other side
The road to UHC will be fraught with risk and will require creative new ideas for reaching the unreached. For one, we must ensure that whatever systems are put in place to expand access to basic health interventions will not inadvertently damage immunization coverage, but will reinforce progress that has been made in expanding immunization coverage.
It is also clear that the achievement of UHC goals by 2030, or by any time, will require us to not only expand and improve upon the health systems that already exist, but also to change our approach to these imperfect health systems. Those families who receive no basic health services are called “hard to reach” for a reason. The challenge in devising a system flexible and comprehensive enough to reach everyone is very real, and very worthwhile.
Despite tremendous global progress, diarrhea remains the second leading infectious cause of under-5 deaths, taking a child’s life almost every minute. Although diarrhea can seem like a common, simple childhood ailment in many places, a single episode of diarrhea can be serious, even deadly, and have severe economic implications for families and communities. Advocates play a critical role in ensuring evidence-based diarrhea prevention and control programs and policies are a top priority globally and in the countries where this disease is most prolific.
How preventing diarrhea can protect children, families, communities, and health systems
Despite tremendous global progress, diarrhea remains the second leading infectious cause of under-5 deaths, taking a child’s life almost every minute.[1],[2] Although diarrhea can seem like a common, simple childhood ailment, in many places a single episode of diarrhea can be serious, even deadly, and have severe economic implications for families and communities.
Repeated, prolonged diarrhea can have lasting – but sometimes overlooked – impacts on child health and development.
Treating diarrhea can be costly to families and health systems, and treatment costs can even push some families into poverty.
Rotavirus causes approximately one third of diarrhea deaths, and is only adequately preventable via vaccination – water, sanitation, and hygiene interventions that work to prevent other types of diarrhea don’t work to prevent rotavirus.
Cholera vaccination is used to stop endemic cholera and respond to cholera outbreaks, which are common in humanitarian emergency settings.
Advocates play a critical role in ensuring evidence-based diarrhea prevention and control programs and policies are a top priority globally and in the countries where the outcomes of diarrheal diseases are most devastating.
The burden of diarrhea globally
Each year, there are an estimated 1 billion episodes of diarrhea with approximately 500,000 deaths in children under five years of age.[1],[2] WHO estimates that children in low- and middle-income countries each have approximately three episodes of diarrhea a year.[3] Although improvements have been made in our efforts to stop diarrhea deaths, we still have far too many episodes: since 1990, the number of diarrhea deaths has decreased by 65%, but the number of new diarrhea episodes has decreased by only 24%.[4] This burden is disproportionally concentrated in low- and middle-income countries, with over half of the diarrheal deaths occurring in sub-Saharan Africa – a low-resource setting where progress is slowest.[5]
The impact of diarrhea on children
Each episode of diarrhea deprives a child of nutrition necessary for growth and contributes to malnutrition, making these children more vulnerable to diarrhea yet less able to fight it.[3] After an episode of diarrhea, children grow less in length than children who did not have diarrhea. When a child has repeated episodes of diarrhea, it can lead to chronic malnutrition and stunting, which in turn is associated with poor functional outcomes such as impaired cognitive development. Prolonged and frequent episodes of diarrhea in young children under the age of two affects them in later childhood and adolescence by leading to delays in school readiness and poor performance in school, as compared to their peers.
Episodes of diarrhea can exacerbate underlying undernutrition and can impair immunity hampering the ability to fight diseases such as pneumonia.[6] During diarrheal episodes, children can lose Vitamin A and zinc, which may predispose some children to pneumonia. In addition, children with more frequent episodes of diarrhea are more likely have chronic health issues later in life, like high blood pressure, which are taxing on both families and health systems.
Tools to defeat diarrhea
Aids to Help Protect and Prevent diarrhea disease and deaths
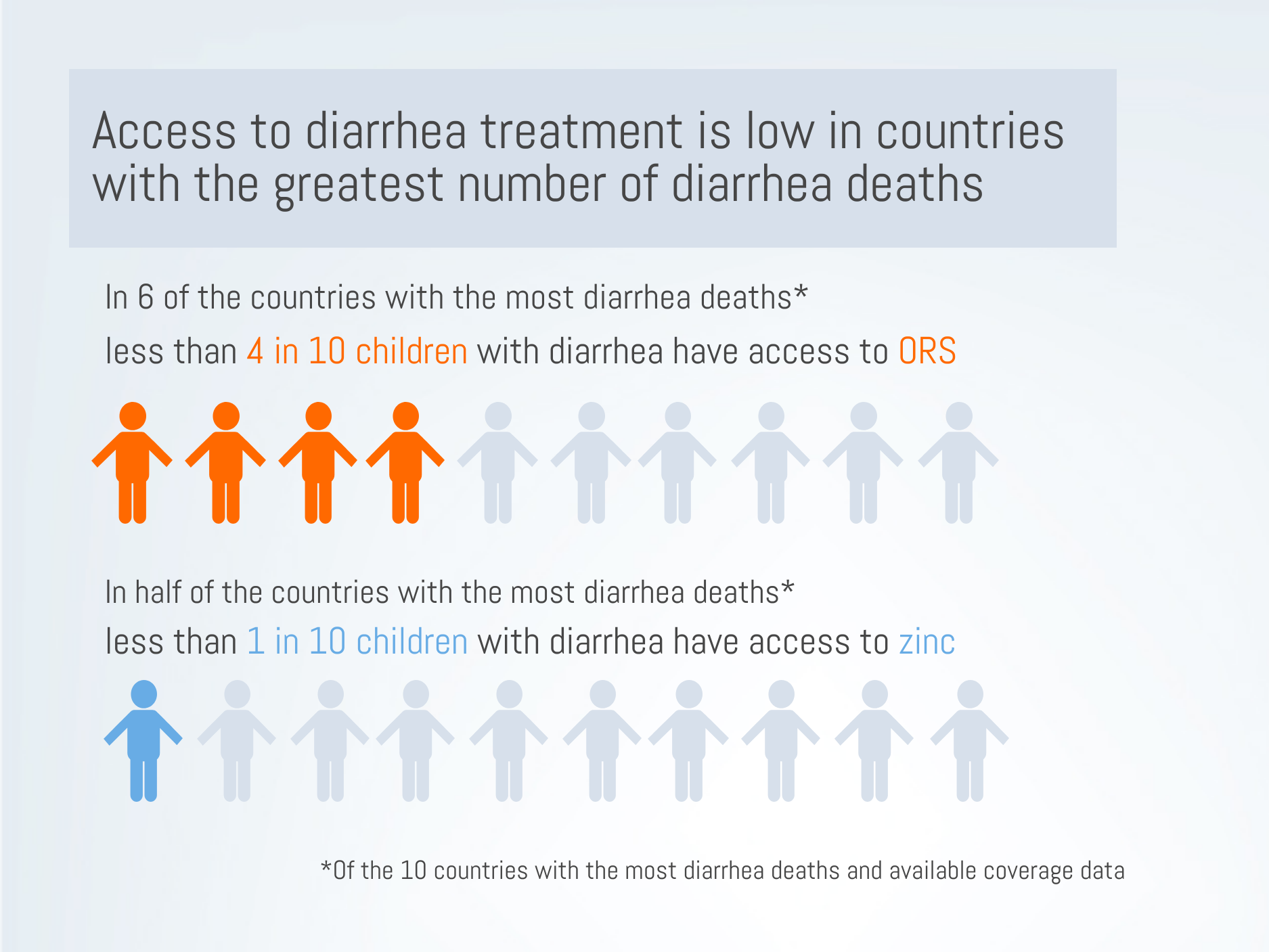
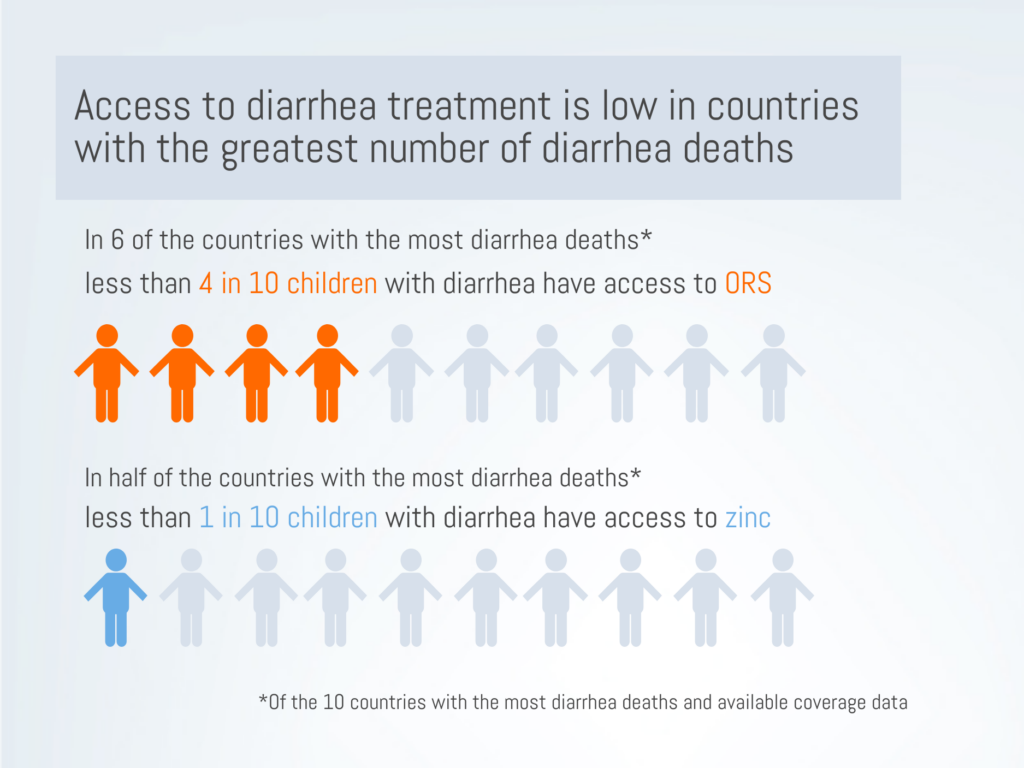
We have highly effective tools to fight diarrhea. Interventions to improve water, sanitation, and hygiene (WASH) have been successful in reducing the number of diarrhea cases.[7] Exclusive breastfeeding for the first 6 months of life can protect infants from undernutrition and its associated vulnerability to diarrhea.[7] Inexpensive but effective treatments like oral rehydration salts (ORS) and zinc supplements work to stop diarrhea episodes from becoming severe and deadly. Yet, access to ORS and zinc is dismally low in many high-burden settings. In 6 of the 10 countries with the highest number of diarrhea deaths[7], national ORS coverage is below 40%.[8] In half of the 10 highest-burden countries[7], fewer than one in ten children have access to zinc supplements. In addition, we also see inequities in access to treatment. In at least half of the 10 highest-burden countries, ORS coverage was at least 10 percentage points lower in rural areas compared to urban areas, or in the poorest 20% of the population compared to the wealthiest 20%.[8]
Vaccination is our strongest protection against vaccine-preventable causes of diarrhea
Two types of common diarrhea are vaccine preventable: rotavirus and cholera. Rotavirus vaccines are especially crucial in preventing a large proportion of diarrhea deaths and hospitalizations around the world. Cholera vaccination is critical in preventing outbreaks in high-risk settings.
Rotavirus vaccination can prevent hospitalizations and death
Although WASH interventions have successfully reduced the global burden of diarrhea, one main cause of diarrhea mortality – rotavirus – is not prevented through WASH interventions.[9],[10] Rotavirus is associated with approximately one third of diarrhea deaths and can only be adequately prevented through vaccination.[2],[9]
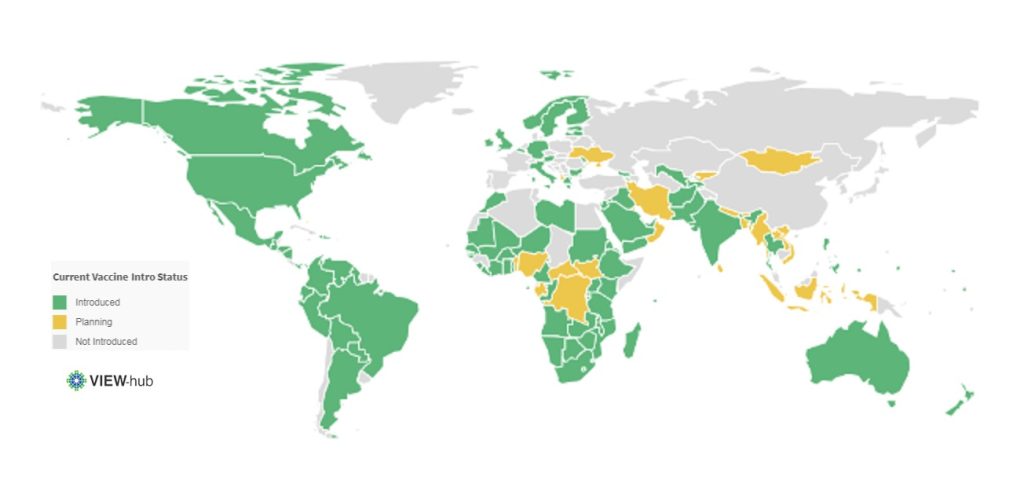
Rotavirus is a leading cause of diarrhea in infants.[5] This highly contagious virus kills about 200,000 children under 5 each year and is responsible for almost 40% of all diarrhea hospitalizations each year.[2],[5] Although ORS can treat simple cases of rotavirus, many of the world’s poorest children don’t have access to ORS.[8] Rotavirus vaccines have proven highly effective and impactful in countries where they have been introduced. In Malawi, for example, there was a 35% decrease in all-cause diarrhea deaths following rotavirus vaccination.[11] Rotavirus hospitalizations in children under 1 year fell by 80% after vaccine introduction.[12] As of January 2019, 97 countries have introduced rotavirus vaccines into their national schedule.[13]
Current Rotavirus Vaccine Introduction Status*
*As of January 2019
Rotavirus vaccination can protect health systems and resources
Although diarrhea treatment is relatively inexpensive, when we factor in the sheer burden of diarrhea, these treatments are costly to health systems and require substantial health worker capacity. Although many cases of diarrhea can be treated in outpatient facilities with low-cost treatment, inpatient treatment of diarrhea can cost hospitals 25 times the cost of outpatient treatment, per patient.[14]
Treating diarrhea uses limited health systems resources, such as hospital beds, and consequently consumes the resources that can be used to treat other diseases – often diseases aren’t preventable. Therefore, direct and indirect benefits of rotavirus vaccination programs play a critical role in reducing the strain on health systems. One in four children who were taken to a large pediatric hospital in Bangladesh were refused admission to the hospital because all of the beds were occupied. Acute diarrhea was one of the most common reasons for being admitted to the hospital, showing children with acute diarrhea filled many of the available hospital beds. Over half of the acute diarrhea cases that were admitted were due to rotavirus, showing that vaccination could prevent children from both needing and utilizing essential hospital resources.
We’ve seen tremendous reductions in hospitalizations for rotavirus diarrhea and all-cause diarrhea following rotavirus vaccine introductions.[15] A review of rotavirus vaccine introductions found that, globally, all-cause diarrhea hospitalizations reduced by almost 40% in children under 5 in regions where the vaccine had been introduced. The continued use and scale up of rotavirus vaccines will alleviate pressure from over-burdened facilities, enabling health systems to be more responsive.
Rotavirus vaccination may protect families from being pushed into poverty due to treatment costs
Rotavirus vaccination programs can protect the most vulnerable families from medical impoverishment and catastrophic healthcare costs. When looking at all-cause diarrhea In Malawi, the costs associated with treating diarrhea pushed families into poverty, with treatment costs exceeding the monthly income for one in six families needing inpatient care and one in ten families needing outpatient care. Families can be pushed into poverty by the costs of hospitalizing a child with rotavirus for several days. In Malaysia, the inpatient costs of rotavirus treatment can cost families 25% of an average family’s monthly income. Direct and indirect treatment costs, such as medicine and transportation, caused almost 9 in 10 Malaysian families to spend more than 10% of their monthly household income on treating rotavirus.
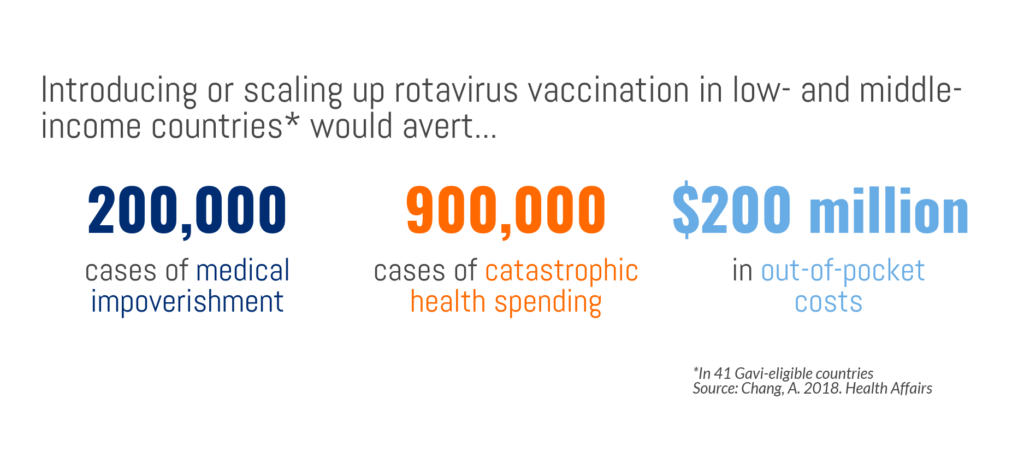
Rotavirus vaccine introduction in 41 GAVI-eligible countries could avert 40% of catastrophic health costs – 900,000 cases – and 40% of medical impoverishment – 200,000 cases. In other words, with rotavirus vaccination programs, 900,000 families would not incur health costs that are higher than a substantial proportion of their income and 200,000 families not would fall below the poverty line due to treatment costs. If rotavirus vaccination programs were introduced or scaled up in Gavi-supported countries, $200 million in out-of-pocket health expenses attributable to severe rotavirus infections could be averted, meaning low-income families would have more disposable income and greater financial stability. With vaccines being one of the more equitable health interventions accessible to poor families, they are an important strategy to reduce the gap in health outcomes by household income as well as protect many families from being pushed into poverty. Inequitable access to treatment, not an uncommon event, only exacerbates the disproportionate risk of mortality in vulnerable children, again underscoring the importance of preventing diarrhea in the first place and protecting children from the vicious aftermath of diarrhea.
Rotavirus vaccination can protect communities
Rotavirus vaccines provide immunity for not only children directly vaccinated but also affords protection to their families and communities. This herd immunity magnifies the public health benefit of rotavirus vaccination by extending protection to those age groups in the population who are not directly receiving the vaccine but can contract and transmit the disease. This additional benefit is essential for a resilient pathogen like rotavirus, that can live on surfaces – and therefore transmit disease – for days. As a result of rotavirus immunized children in the community, rotavirus hospital admissions in unvaccinated children aged two to five years of age, who were not age-eligible to receive the vaccine at the time, were reduced by 41% to 92% in hospitals across the US, showing the profound value of herd immunity.
Cholera vaccination can protect vulnerable groups
Cholera burden
Diarrhea caused by cholera can be rapidly fatal, with as many as 1 in every 5 cases of cholera advances to severe disease.[16] Cholera, often called a disease of poverty, can be endemic and epidemic in settings without strong water and sanitation systems, such as humanitarian emergency settings. Because settings where cholera is most rampant are often those with weak or overburdened health systems, diagnosing and recording cases is difficult; the global estimates of cholera cases each year – between 1.3 and 4 million cases – likely underestimate the true burden.[16]
Unlike many vaccine-preventable diseases, the global number of cholera cases has been steadily climbing for the past 10 years. Devastating cholera epidemics have impacted Yemen, Haiti, Somalia, the Democratic Republic of Congo, and South Sudan in recent years, and continue to be a threat in fragile settings.[17] In addition to the health impacts of cholera, previous outbreaks have led to significant economic losses to countries, caused by reduced revenue on trade and tourism, and continue to threaten countries.[16]
Cholera vaccination
Cholera vaccination is a crucial, cost-effective tool to fight cholera, especially in fragile settings that lack sufficient water and sanitation. In 2013, global partners collaborated to form a stockpile of the oral cholera vaccine, managed by the Global Task Force on Cholera Control and funded by Gavi, the Vaccine Alliance.[16] The stockpile has been utilized for mass vaccination campaigns for prevention in humanitarian crises and for reactive response to outbreaks.[17]
An important – and beneficial – feature of cholera is that vaccinating a relatively small number of people can result in significant herd protection. Research from Bangladesh suggests that 70% vaccine coverage can stop cholera transmission, which greatly amplifies the impact of vaccine campaigns and investments.[18] Cholera vaccination is also a critical tool in managing outbreaks and protecting national and global health security.
Continuing – and strengthening – the fight against diarrheal diseases
Certain types of serious diarrhea can be both preventable and treatable, and a large proportion of child diarrhea deaths can be prevented through vaccination. We have the tools to defeat diarrhea, but these tools are only effective when backed by strong political and financial commitment. The global fight against childhood diarrhea has undoubtedly had a profound impact on child health and broader societal development. Yet, consistently low treatment coverage and constraints in vaccine supply highlight ongoing challenges. These challenges must be responded to with the resources and commitment necessary to pick up the pace of progress, so we can be stronger in the global fight against one of the most common causes of childhood illness and death.
[4] Troeger, C., Colombara, D. V., Rao, P. C., Khalil, I. A., Brown, A., Brewer, T. G., … & Petri, W. A. (2018). Global disability-adjusted life-year estimates of long-term health burden and undernutrition attributable to diarrhoeal diseases in children younger than 5 years. The Lancet Global Health, 6(3), e255-e269.
[5] Tate, J. E., Burton, A. H., Boschi-Pinto, C., Parashar, U. D., World Health Organization–Coordinated Global Rotavirus Surveillance Network, Agocs, M., … & Ranjan Wijesinghe, P. (2016). Global, regional, and national estimates of rotavirus mortality in children< 5 years of age, 2000–2013. Clinical Infectious Diseases, 62(suppl_2), S96-S105.
[6] Ibrahim, M. K., Zambruni, M., Melby, C. L., & Melby, P. C. (2017). Impact of childhood malnutrition on host defense and infection. Clinical microbiology reviews, 30(4), 919-971.
[8] International Vaccine Access Center (IVAC), Johns Hopkins Bloomberg School of Public Health. (2018). Pneumonia and Diarrhea Progress Report 2018.
[9] Lamberti, L. M., Ashraf, S., Walker, C. L. F., & Black, R. E. (2016). A systematic review of the effect of rotavirus vaccination on diarrhea outcomes among children younger than 5 years. The Pediatric infectious disease journal, 35(9), 992-998.
[10] Glass, R. I., Parashar, U., Patel, M., Gentsch, J., & Jiang, B. (2014). Rotavirus vaccines: successes and challenges. Journal of infection, 68, S9-S18.
[11] Bar-Zeev, N., King, C., Phiri, T., Beard, J., Mvula, H., Crampin, A. C., … & Costello, A. (2018). Impact of monovalent rotavirus vaccine on diarrhoea-associated post-neonatal infant mortality in rural communities in Malawi: a population-based birth cohort study. The Lancet Global Health, 6(9), e1036-e1044.
[12] Burnett, E., Jonesteller, C. L., Tate, J. E., et al. 2017. Global impact of rotavirus vaccination on childhood hospitalizations and mortality from diarrhea.. The Journal of Infectious Diseases. 215(11), 1666-1672..
[13] International Vaccine Access Center (2018). VIEW-hub: Vaccine Introduction and Epidemiology Window. Retreived from: http://view-hub.org. Accessed January 31, 2018.
[14] Sarker, A. R., Sultana, M., Mahumud, R. A., Ali, N., Huda, T. M., Haider, S., … & Morton, A. (2018). Economic costs of hospitalized diarrheal disease in Bangladesh: a societal perspective. Global health research and policy, 3(1), 1.
[15] Groome, M. J., Zell, E. R., Solomon, F., Nzenze, S., Parashar, U. D., Izu, A., & Madhi, S. A. (2016). Temporal association of rotavirus vaccine introduction and reduction in all-cause childhood diarrheal hospitalizations in South Africa. Clinical Infectious Diseases, 62(suppl_2), S188-S195.
[16] World Health Organization. (2017). Cholera vaccines: WHO position paper–August 2017. Weekly Epidemiological Record. 92(34), 477-498.
[17] Wierzba, T. F. (2018). Oral cholera vaccines and their impact on the global burden of disease. Human vaccines & immunotherapeutics, 1-8.
[18] Dimitrov, D. T., Troeger, C., Halloran, M. E., Longini, I. M., & Chao, D. L. (2014). Comparative effectiveness of different strategies of oral cholera vaccination in Bangladesh: a modeling study. PLoS neglected tropical diseases, 8(12), e3343.