December 12th is worldwide Universal Health Coverage (UHC) day! Although exceedingly complex in its implementation, the concept behind UHC is simple: All people should benefit from quality health services, medicines and vaccinations, and no one should be put in financial peril to do so. In recognition of UHC Day 2018, the VoICE team brings you a brief look at the interplay between coverage of immunization and other basic health interventions, and the important role of immunization in protecting against financial risk – both within the context of the Sustainable Development Goal Target for UHC.
Achieving universal coverage of basic health services will require strengthening and expanding current health systems AND new approaches to reaching those who still cannot or do not access health services.
The reach of immunization delivery programs can be leveraged to provide other basic services – and increase financial efficiency of health systems – and the reverse is also true: the delivery of other interventions can help to increase the uptake of vaccines.
Achievement of UHC will positively contribute to at least six of the 17 Sustainable Development Goals.
Immunization can contribute significantly to achieving financial risk protection against health costs.
Universal Health Coverage and the Sustainable Development Goals
December 12th is worldwide Universal Health Coverage (UHC) day! The aim of drawing attention to this day is to shine the global spotlight on the gaps in achieving health as a human right. Although exceedingly complex in its implementation, the concept behind UHC is simple: All people should benefit from quality health services, medicines and vaccinations, and no one should be put in financial peril to do so.
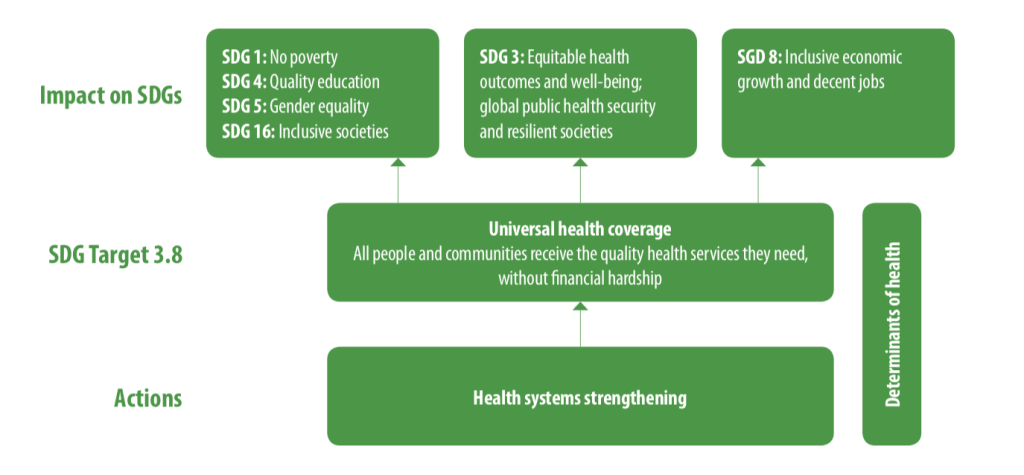
In 2015, 193 United Nations Member States committed to an ambitious set of 17 “Sustainable Development Goals” (SDGs) by 2030. The right to health not only figures prominently as a goal in and of itself – SDG3 is to “Ensure healthy lives and promote well-being for all at all ages” – but is also fundamentally intertwined with goals related to equity, poverty, economic growth and inclusion. (See Figure 1.)
Figure 1: The interrelatedness of Universal Health Coverage with other Sustainable Development Goals, and the importance of health systems strengthening.
Source: Tracking Universal Health Coverage: 2017 Global Monitoring Report.World Health Organization and International Bank for Reconstruction and Development / The World Bank; 2017. License: CC BY-NC-SA 3.0 IGO. Available here: http://www.who.int/healthinfo/universal_health_coverage/report/2017/en/
Embodied in the 8th Target of SDG3 (SDG 3.8), the pursuit of UHC is supported by the twin indicators of 1) coverage of essential services (including immunization), and 2) financial risk protection from the incurrence of economically burdensome health costs. In recognition of UHC Day 2018, the VoICE team brings you a brief look at the interplay between coverage of immunization and other basic health interventions, and the important role of immunization in protecting against financial risk – both within the context of SDG 3.8.
Building on coverage of vaccines gives UHC a head start, but there is more to do
Equity is at the heart of the Sustainable Development Goal target 3.8, which seeks to achieve universal health coverage and financial risk protection for all. The coverage indicator for the achievement of UHC tracks the coverage of 14 “tracer interventions”, which together serve as a barometer for access to basic health services. Access to immunization is tracked through the coverage of the third dose of DTP3, one of four maternal and child health tracer interventions. Although DTP3 coverage is evidence of the fact that immunization is one of the most widely available and equitably distributed interventions worldwide, several other important vaccines lag behind the 85% coverage of DTP3 worldwide in 2017.
Specific vaccines notwithstanding, high coverage with some vaccines such as DTP make immunization programs a critical backbone of any universal health coverage strategy. Routine and campaign-based immunization programs reach some children in remote or poverty stricken areas whose families have little other connection to the health system, and as such, offer opportunities to provide additional basic health care services to children and their families, especially interventions associated with maternal and child health. See Figure 2 for some highlights from VoICE of the opportunities for mutual reinforcement between immunization and other programs.
Figure 2: Examples of the integration of immunization and other health services.
Vitamin A distribution integrated with polio vaccine campaigns led to increased VitA coverage in several African countries.
Delivery of HPV vaccine to school-age girls in Rwanda provided an opportunity to offer school-age boys a variety of health services at the same time.
The timing of childhood immunizations could be harnessed to deliver a range of early childhood development interventions such as newborn hearing screening, sickle cell screening, treatment and surveillance, maternal education around key newborn care issues such as jaundice, and tracking early signs of poor growth and nutrition.
Despite the relatively high coverage globally of some vaccines, other critical vaccines have reached only a small fraction of the world’s children. Fully 15% of the world’s children are not reached at all by immunization – a gap whose distribution carries significant inequity – so vaccine coverage successes are very much tied to the achievement of UHC goals and targets for other health services.
The achievement of UHC targets will, however, require significant reform and expansion of existing health systems to address challenges such as missed opportunities to integrate services. For example, a recent study in 14 low- and middle-income countries found an exceedingly high rate of missed opportunities to vaccinate in 8 of the 14 countries, despite families coming into contact with the health system. For these countries, children failed to be vaccinated more than 50% of the time, despite they or their mother having received at least one of 5 other basic health interventions provided through the health system. Additionally, for the millions of families not reached at all by current health systems, barriers may include socio-cultural factors, in addition to geography, education, poverty, etc.
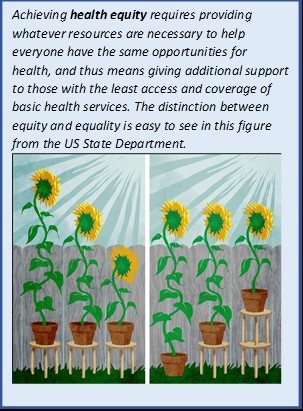
For these families and others with inadequate health services, a truly equity-driven approach is needed. That is, governments, partners, health-providers, and systems will need find ways to provide whatever additional support is needed to help them catch up, not just make the same resources available to everyone.
For families, financial barriers to immunization are relatively low, but health and economic returns are high
The second indicator of the universal health coverage target acknowledges that the costs associated with health care – both preventative services and treatment for illness – are a significant barrier for hundreds of millions of people around the world. These costs prevent some people from even trying to access health services, and for those who do seek care they cannot afford, the financial burden of these services can have significant, negative and lasting economic impact. The provision of a basic package of preventative services, including immunization, would thus create a positive, reinforcing cycle of increased health-seeking behavior and improved financial stability for individuals, families and economies.
Immunization is a critical element to success for two reasons. First, thanks to global institutions such as Gavi and UNICEF, immunization is free of charge for a large proportion of families in the world’s middle and low-income nations and financial barriers to access are thus relatively low. However, not all crucial vaccines are yet available through national immunization programs in every country. In some places, lifesaving vaccines against disease such as pneumococcal disease are only available through the private market, carrying a price tag far too high for many families to access. And, as mentioned above, sociocultural factors and other issues are significant drivers of gaps in vaccine coverage and these must be addressed carefully and concertedly.
The second reason immunization is critical to meeting the financial risk protection targets of UHC is much more obvious: the widespread use of vaccines has the power to avert significant costs associated with treatment of infections. The huge economic burden of these infections stems from the costs associated with treating relatively low-cost but frequently occurring infections and complicated infections such as meningitis which are rare but very expensive to treat. These vaccine-preventable episodes of illness are responsible for a large number of families being pushed into poverty each year.
The hurdles that remain are high, but health for all awaits on the other side
The road to UHC will be fraught with risk and will require creative new ideas for reaching the unreached. For one, we must ensure that whatever systems are put in place to expand access to basic health interventions will not inadvertently damage immunization coverage, but will reinforce progress that has been made in expanding immunization coverage.
It is also clear that the achievement of UHC goals by 2030, or by any time, will require us to not only expand and improve upon the health systems that already exist, but also to change our approach to these imperfect health systems. Those families who receive no basic health services are called “hard to reach” for a reason. The challenge in devising a system flexible and comprehensive enough to reach everyone is very real, and very worthwhile.
Despite tremendous global progress, diarrhea remains the second leading infectious cause of under-5 deaths, taking a child’s life almost every minute. Although diarrhea can seem like a common, simple childhood ailment in many places, a single episode of diarrhea can be serious, even deadly, and have severe economic implications for families and communities. Advocates play a critical role in ensuring evidence-based diarrhea prevention and control programs and policies are a top priority globally and in the countries where this disease is most prolific.
How preventing diarrhea can protect children, families, communities, and health systems
Despite tremendous global progress, diarrhea remains the second leading infectious cause of under-5 deaths, taking a child’s life almost every minute.[1],[2] Although diarrhea can seem like a common, simple childhood ailment, in many places a single episode of diarrhea can be serious, even deadly, and have severe economic implications for families and communities.
Repeated, prolonged diarrhea can have lasting – but sometimes overlooked – impacts on child health and development.
Treating diarrhea can be costly to families and health systems, and treatment costs can even push some families into poverty.
Rotavirus causes approximately one third of diarrhea deaths, and is only adequately preventable via vaccination – water, sanitation, and hygiene interventions that work to prevent other types of diarrhea don’t work to prevent rotavirus.
Cholera vaccination is used to stop endemic cholera and respond to cholera outbreaks, which are common in humanitarian emergency settings.
Advocates play a critical role in ensuring evidence-based diarrhea prevention and control programs and policies are a top priority globally and in the countries where the outcomes of diarrheal diseases are most devastating.
The burden of diarrhea globally
Each year, there are an estimated 1 billion episodes of diarrhea with approximately 500,000 deaths in children under five years of age.[1],[2] WHO estimates that children in low- and middle-income countries each have approximately three episodes of diarrhea a year.[3] Although improvements have been made in our efforts to stop diarrhea deaths, we still have far too many episodes: since 1990, the number of diarrhea deaths has decreased by 65%, but the number of new diarrhea episodes has decreased by only 24%.[4] This burden is disproportionally concentrated in low- and middle-income countries, with over half of the diarrheal deaths occurring in sub-Saharan Africa – a low-resource setting where progress is slowest.[5]
The impact of diarrhea on children
Each episode of diarrhea deprives a child of nutrition necessary for growth and contributes to malnutrition, making these children more vulnerable to diarrhea yet less able to fight it.[3] After an episode of diarrhea, children grow less in length than children who did not have diarrhea. When a child has repeated episodes of diarrhea, it can lead to chronic malnutrition and stunting, which in turn is associated with poor functional outcomes such as impaired cognitive development. Prolonged and frequent episodes of diarrhea in young children under the age of two affects them in later childhood and adolescence by leading to delays in school readiness and poor performance in school, as compared to their peers.
Episodes of diarrhea can exacerbate underlying undernutrition and can impair immunity hampering the ability to fight diseases such as pneumonia.[6] During diarrheal episodes, children can lose Vitamin A and zinc, which may predispose some children to pneumonia. In addition, children with more frequent episodes of diarrhea are more likely have chronic health issues later in life, like high blood pressure, which are taxing on both families and health systems.
Tools to defeat diarrhea
Aids to Help Protect and Prevent diarrhea disease and deaths
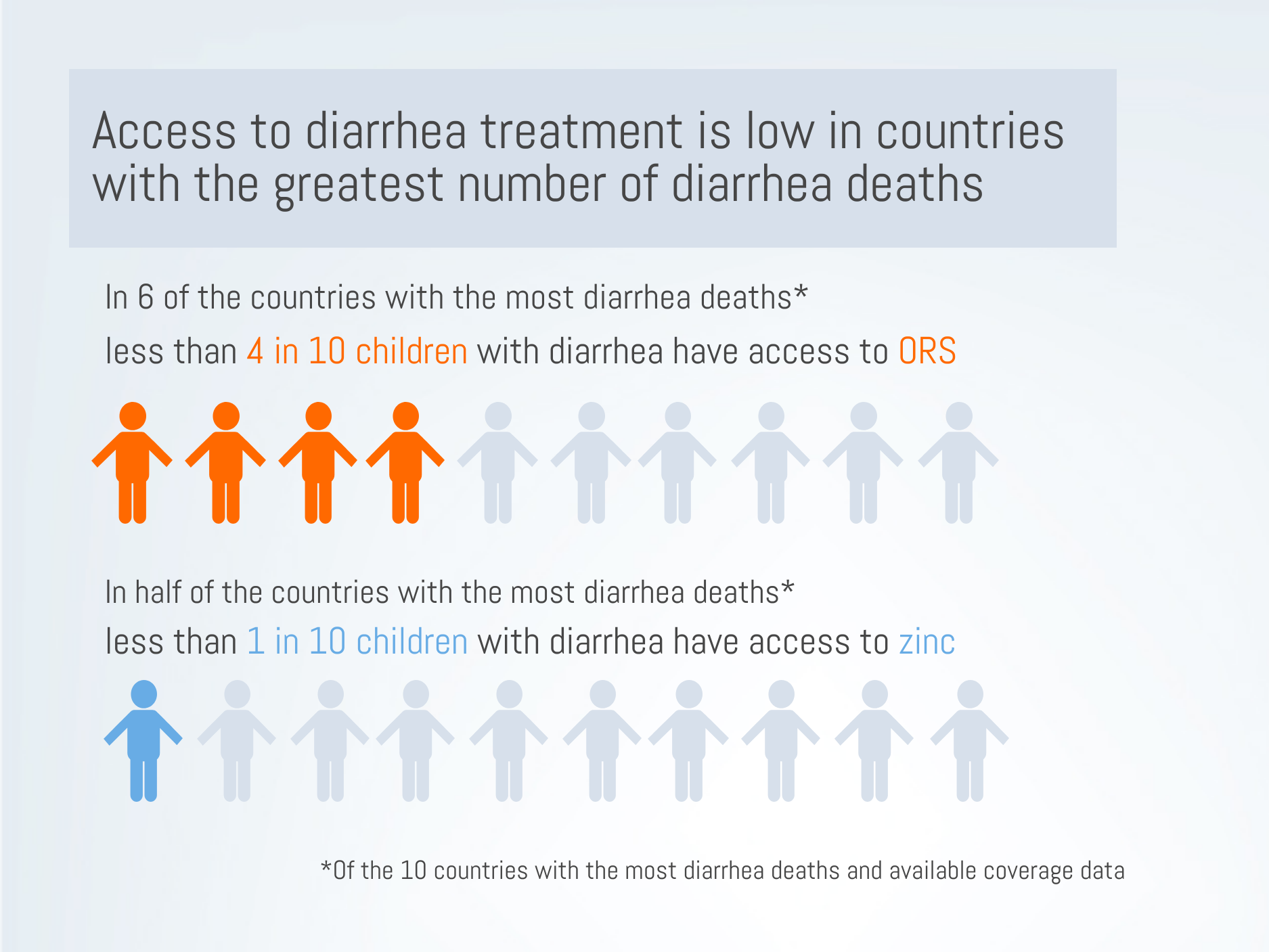
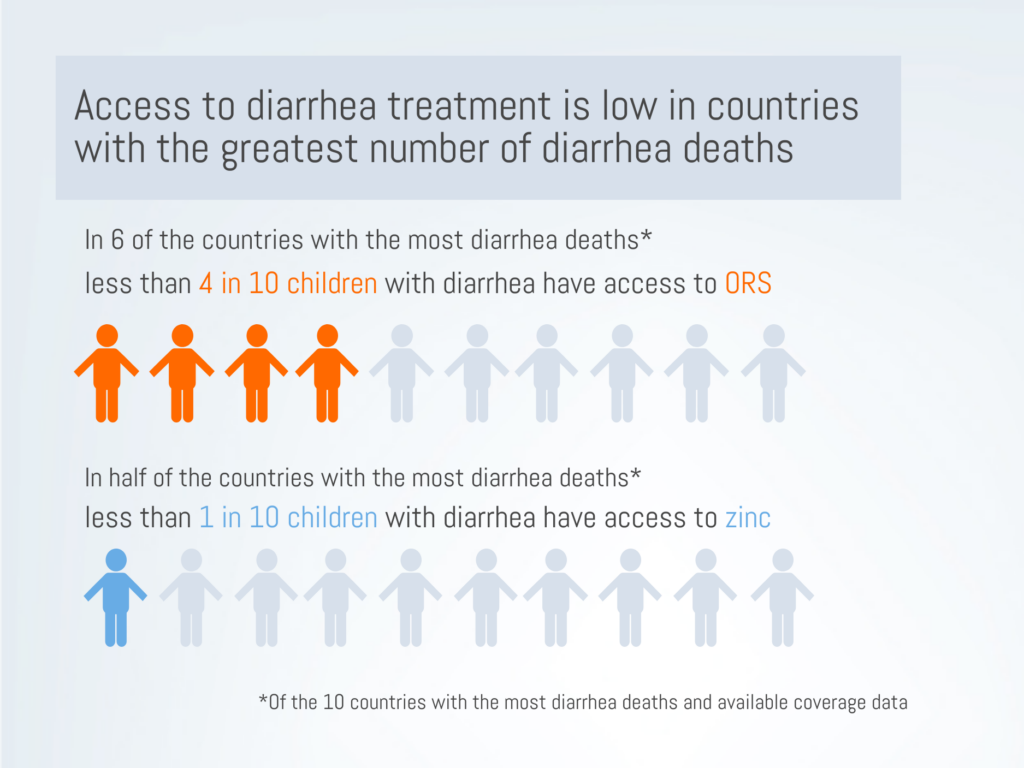
We have highly effective tools to fight diarrhea. Interventions to improve water, sanitation, and hygiene (WASH) have been successful in reducing the number of diarrhea cases.[7] Exclusive breastfeeding for the first 6 months of life can protect infants from undernutrition and its associated vulnerability to diarrhea.[7] Inexpensive but effective treatments like oral rehydration salts (ORS) and zinc supplements work to stop diarrhea episodes from becoming severe and deadly. Yet, access to ORS and zinc is dismally low in many high-burden settings. In 6 of the 10 countries with the highest number of diarrhea deaths[7], national ORS coverage is below 40%.[8] In half of the 10 highest-burden countries[7], fewer than one in ten children have access to zinc supplements. In addition, we also see inequities in access to treatment. In at least half of the 10 highest-burden countries, ORS coverage was at least 10 percentage points lower in rural areas compared to urban areas, or in the poorest 20% of the population compared to the wealthiest 20%.[8]
Vaccination is our strongest protection against vaccine-preventable causes of diarrhea
Two types of common diarrhea are vaccine preventable: rotavirus and cholera. Rotavirus vaccines are especially crucial in preventing a large proportion of diarrhea deaths and hospitalizations around the world. Cholera vaccination is critical in preventing outbreaks in high-risk settings.
Rotavirus vaccination can prevent hospitalizations and death
Although WASH interventions have successfully reduced the global burden of diarrhea, one main cause of diarrhea mortality – rotavirus – is not prevented through WASH interventions.[9],[10] Rotavirus is associated with approximately one third of diarrhea deaths and can only be adequately prevented through vaccination.[2],[9]
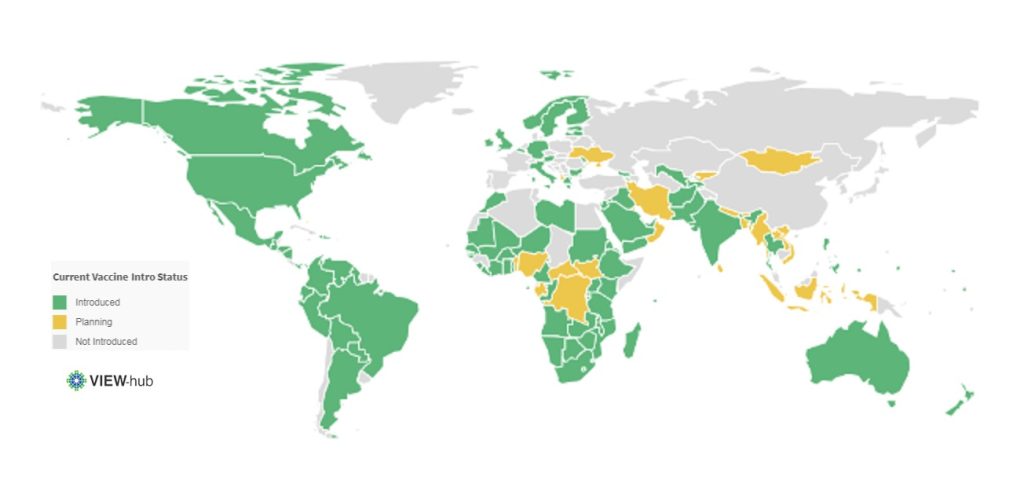
Rotavirus is a leading cause of diarrhea in infants.[5] This highly contagious virus kills about 200,000 children under 5 each year and is responsible for almost 40% of all diarrhea hospitalizations each year.[2],[5] Although ORS can treat simple cases of rotavirus, many of the world’s poorest children don’t have access to ORS.[8] Rotavirus vaccines have proven highly effective and impactful in countries where they have been introduced. In Malawi, for example, there was a 35% decrease in all-cause diarrhea deaths following rotavirus vaccination.[11] Rotavirus hospitalizations in children under 1 year fell by 80% after vaccine introduction.[12] As of January 2019, 97 countries have introduced rotavirus vaccines into their national schedule.[13]
Current Rotavirus Vaccine Introduction Status*
*As of January 2019
Rotavirus vaccination can protect health systems and resources
Although diarrhea treatment is relatively inexpensive, when we factor in the sheer burden of diarrhea, these treatments are costly to health systems and require substantial health worker capacity. Although many cases of diarrhea can be treated in outpatient facilities with low-cost treatment, inpatient treatment of diarrhea can cost hospitals 25 times the cost of outpatient treatment, per patient.[14]
Treating diarrhea uses limited health systems resources, such as hospital beds, and consequently consumes the resources that can be used to treat other diseases – often diseases aren’t preventable. Therefore, direct and indirect benefits of rotavirus vaccination programs play a critical role in reducing the strain on health systems. One in four children who were taken to a large pediatric hospital in Bangladesh were refused admission to the hospital because all of the beds were occupied. Acute diarrhea was one of the most common reasons for being admitted to the hospital, showing children with acute diarrhea filled many of the available hospital beds. Over half of the acute diarrhea cases that were admitted were due to rotavirus, showing that vaccination could prevent children from both needing and utilizing essential hospital resources.
We’ve seen tremendous reductions in hospitalizations for rotavirus diarrhea and all-cause diarrhea following rotavirus vaccine introductions.[15] A review of rotavirus vaccine introductions found that, globally, all-cause diarrhea hospitalizations reduced by almost 40% in children under 5 in regions where the vaccine had been introduced. The continued use and scale up of rotavirus vaccines will alleviate pressure from over-burdened facilities, enabling health systems to be more responsive.
Rotavirus vaccination may protect families from being pushed into poverty due to treatment costs
Rotavirus vaccination programs can protect the most vulnerable families from medical impoverishment and catastrophic healthcare costs. When looking at all-cause diarrhea In Malawi, the costs associated with treating diarrhea pushed families into poverty, with treatment costs exceeding the monthly income for one in six families needing inpatient care and one in ten families needing outpatient care. Families can be pushed into poverty by the costs of hospitalizing a child with rotavirus for several days. In Malaysia, the inpatient costs of rotavirus treatment can cost families 25% of an average family’s monthly income. Direct and indirect treatment costs, such as medicine and transportation, caused almost 9 in 10 Malaysian families to spend more than 10% of their monthly household income on treating rotavirus.
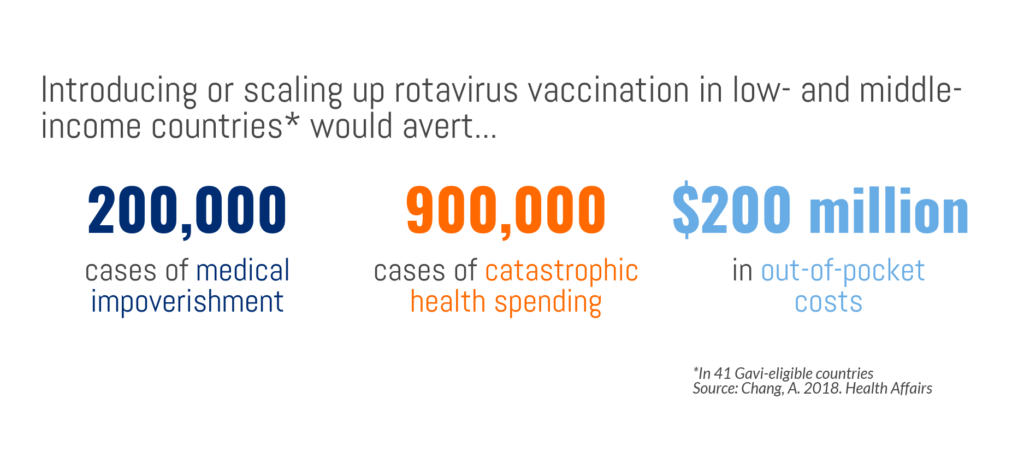
Rotavirus vaccine introduction in 41 GAVI-eligible countries could avert 40% of catastrophic health costs – 900,000 cases – and 40% of medical impoverishment – 200,000 cases. In other words, with rotavirus vaccination programs, 900,000 families would not incur health costs that are higher than a substantial proportion of their income and 200,000 families not would fall below the poverty line due to treatment costs. If rotavirus vaccination programs were introduced or scaled up in Gavi-supported countries, $200 million in out-of-pocket health expenses attributable to severe rotavirus infections could be averted, meaning low-income families would have more disposable income and greater financial stability. With vaccines being one of the more equitable health interventions accessible to poor families, they are an important strategy to reduce the gap in health outcomes by household income as well as protect many families from being pushed into poverty. Inequitable access to treatment, not an uncommon event, only exacerbates the disproportionate risk of mortality in vulnerable children, again underscoring the importance of preventing diarrhea in the first place and protecting children from the vicious aftermath of diarrhea.
Rotavirus vaccination can protect communities
Rotavirus vaccines provide immunity for not only children directly vaccinated but also affords protection to their families and communities. This herd immunity magnifies the public health benefit of rotavirus vaccination by extending protection to those age groups in the population who are not directly receiving the vaccine but can contract and transmit the disease. This additional benefit is essential for a resilient pathogen like rotavirus, that can live on surfaces – and therefore transmit disease – for days. As a result of rotavirus immunized children in the community, rotavirus hospital admissions in unvaccinated children aged two to five years of age, who were not age-eligible to receive the vaccine at the time, were reduced by 41% to 92% in hospitals across the US, showing the profound value of herd immunity.
Cholera vaccination can protect vulnerable groups
Cholera burden
Diarrhea caused by cholera can be rapidly fatal, with as many as 1 in every 5 cases of cholera advances to severe disease.[16] Cholera, often called a disease of poverty, can be endemic and epidemic in settings without strong water and sanitation systems, such as humanitarian emergency settings. Because settings where cholera is most rampant are often those with weak or overburdened health systems, diagnosing and recording cases is difficult; the global estimates of cholera cases each year – between 1.3 and 4 million cases – likely underestimate the true burden.[16]
Unlike many vaccine-preventable diseases, the global number of cholera cases has been steadily climbing for the past 10 years. Devastating cholera epidemics have impacted Yemen, Haiti, Somalia, the Democratic Republic of Congo, and South Sudan in recent years, and continue to be a threat in fragile settings.[17] In addition to the health impacts of cholera, previous outbreaks have led to significant economic losses to countries, caused by reduced revenue on trade and tourism, and continue to threaten countries.[16]
Cholera vaccination
Cholera vaccination is a crucial, cost-effective tool to fight cholera, especially in fragile settings that lack sufficient water and sanitation. In 2013, global partners collaborated to form a stockpile of the oral cholera vaccine, managed by the Global Task Force on Cholera Control and funded by Gavi, the Vaccine Alliance.[16] The stockpile has been utilized for mass vaccination campaigns for prevention in humanitarian crises and for reactive response to outbreaks.[17]
An important – and beneficial – feature of cholera is that vaccinating a relatively small number of people can result in significant herd protection. Research from Bangladesh suggests that 70% vaccine coverage can stop cholera transmission, which greatly amplifies the impact of vaccine campaigns and investments.[18] Cholera vaccination is also a critical tool in managing outbreaks and protecting national and global health security.
Continuing – and strengthening – the fight against diarrheal diseases
Certain types of serious diarrhea can be both preventable and treatable, and a large proportion of child diarrhea deaths can be prevented through vaccination. We have the tools to defeat diarrhea, but these tools are only effective when backed by strong political and financial commitment. The global fight against childhood diarrhea has undoubtedly had a profound impact on child health and broader societal development. Yet, consistently low treatment coverage and constraints in vaccine supply highlight ongoing challenges. These challenges must be responded to with the resources and commitment necessary to pick up the pace of progress, so we can be stronger in the global fight against one of the most common causes of childhood illness and death.
[4] Troeger, C., Colombara, D. V., Rao, P. C., Khalil, I. A., Brown, A., Brewer, T. G., … & Petri, W. A. (2018). Global disability-adjusted life-year estimates of long-term health burden and undernutrition attributable to diarrhoeal diseases in children younger than 5 years. The Lancet Global Health, 6(3), e255-e269.
[5] Tate, J. E., Burton, A. H., Boschi-Pinto, C., Parashar, U. D., World Health Organization–Coordinated Global Rotavirus Surveillance Network, Agocs, M., … & Ranjan Wijesinghe, P. (2016). Global, regional, and national estimates of rotavirus mortality in children< 5 years of age, 2000–2013. Clinical Infectious Diseases, 62(suppl_2), S96-S105.
[6] Ibrahim, M. K., Zambruni, M., Melby, C. L., & Melby, P. C. (2017). Impact of childhood malnutrition on host defense and infection. Clinical microbiology reviews, 30(4), 919-971.
[8] International Vaccine Access Center (IVAC), Johns Hopkins Bloomberg School of Public Health. (2018). Pneumonia and Diarrhea Progress Report 2018.
[9] Lamberti, L. M., Ashraf, S., Walker, C. L. F., & Black, R. E. (2016). A systematic review of the effect of rotavirus vaccination on diarrhea outcomes among children younger than 5 years. The Pediatric infectious disease journal, 35(9), 992-998.
[10] Glass, R. I., Parashar, U., Patel, M., Gentsch, J., & Jiang, B. (2014). Rotavirus vaccines: successes and challenges. Journal of infection, 68, S9-S18.
[11] Bar-Zeev, N., King, C., Phiri, T., Beard, J., Mvula, H., Crampin, A. C., … & Costello, A. (2018). Impact of monovalent rotavirus vaccine on diarrhoea-associated post-neonatal infant mortality in rural communities in Malawi: a population-based birth cohort study. The Lancet Global Health, 6(9), e1036-e1044.
[12] Burnett, E., Jonesteller, C. L., Tate, J. E., et al. 2017. Global impact of rotavirus vaccination on childhood hospitalizations and mortality from diarrhea.. The Journal of Infectious Diseases. 215(11), 1666-1672..
[13] International Vaccine Access Center (2018). VIEW-hub: Vaccine Introduction and Epidemiology Window. Retreived from: http://view-hub.org. Accessed January 31, 2018.
[14] Sarker, A. R., Sultana, M., Mahumud, R. A., Ali, N., Huda, T. M., Haider, S., … & Morton, A. (2018). Economic costs of hospitalized diarrheal disease in Bangladesh: a societal perspective. Global health research and policy, 3(1), 1.
[15] Groome, M. J., Zell, E. R., Solomon, F., Nzenze, S., Parashar, U. D., Izu, A., & Madhi, S. A. (2016). Temporal association of rotavirus vaccine introduction and reduction in all-cause childhood diarrheal hospitalizations in South Africa. Clinical Infectious Diseases, 62(suppl_2), S188-S195.
[16] World Health Organization. (2017). Cholera vaccines: WHO position paper–August 2017. Weekly Epidemiological Record. 92(34), 477-498.
[17] Wierzba, T. F. (2018). Oral cholera vaccines and their impact on the global burden of disease. Human vaccines & immunotherapeutics, 1-8.
[18] Dimitrov, D. T., Troeger, C., Halloran, M. E., Longini, I. M., & Chao, D. L. (2014). Comparative effectiveness of different strategies of oral cholera vaccination in Bangladesh: a modeling study. PLoS neglected tropical diseases, 8(12), e3343.
Last month at the G7 meeting in Canada, global leaders met to consider gender equality, one of the 5 key themes Canada will advance during their tenure. Partners, experts and representatives in the immunization world echoed this emphasis on gender at the Global Immunization Meeting in Kigali, Rwanda just a few days ago. The issues of gender and gender equity within immunization are complex, and designing research to study equity gaps can be difficult. To understand what we do know about immunization and gender, women’s empowerment and gender equity, the VoICE team this month features an overview of these issues.
Global and national level estimates of vaccine coverage obscure persistent gender inequity in some populations.
At the national level, gender inequality for women is correlated with higher child mortality and lower childhood immunization rates.
Reaching higher levels of education greatly increases the likelihood that a woman’s children will be vaccinated.
The more empowered women are – i.e. have control over family decision-making, financial resources, etc. – the more likely their children are to be vaccinated.
An equity approach to immunization and child health is both a moral imperative and an efficient use of resources.
Equity matters for the health of women and children
While much progress has been made to reduce child mortality and increase vaccine coverage in the last few decades, inequities still exist from a variety of perspectives, and gender influences vaccine access in several ways. When considering both between and within country inequities; geographic, wealth, and educational for example, female specific gender inequity remains a common thread.
In some parts of the world, gender influences a child’s access to vaccines and health care.
Differential vaccine coverage of childhood immunization between boys and girls is an inequity largely invisible at the global level but which persists in certain geographic and social settings. This is reported in studies from regions of the world where there is strong cultural preference for sons over daughters. A study conducted in the urban poor in India which examined household and neighborhood-level determinants of childhood immunization, researchers found that girls were 22% less likely than boys to be fully immunized. This trend has not changed despite increasing overall vaccine coverage rates nationally.
Another study that examined the gender gap in immunization coverage in a rural sub-district of Bangladesh showed that although poverty, low maternal education, and larger number of children in a family decreased the likelihood that any child would be vaccinated, the effect of these factors was more pronounced for girls than for boys. In other words, given the same set of pressures on families that negatively impact immunization, girls fared worse than boys in terms of likelihood of receiving vaccines.
There is a small amount of evidence that girls have less access to care if sick in specific settings. In an Indian study from the northern state of Bihar, girls who were ill were less likely to receive care in a health facility than boys, although the study did not find different rates of immunization coverage between the sexes.
Gender differences in child health care utilization for both prevention and treatment of disease may be a contributing factor driving excess mortality for girls in South Asia. South Asia is the only region of the world in which a slight natural survival advantage in female infants compared to male infants is reversed. This means that in South Asia, male infants have a better chance of surviving to their first birthday than females. It is estimated that the excess female infant mortality in India results in 9 additional deaths/1000 live births of girls compared to boys, and this disparity has worsened since 1990.1
Critically, it must be acknowledged that local attitudes and motives that underpin vaccination and health seeking behaviors can vary significantly between countries and communities and are often driven by a set of complex interrelated factors that, in addition to gender, include parental education, socioeconomic status, geographic access, cultural preferences and biases.
Mothers and childhood immunization
Mariam (pictured left of frame in the green and yellow skirt) a community influencer who lives in Anguar Hausawa and helps to co-ordinate vaccine drives chats to local mothers about vaccination and health issues.
Gender equality for women, and maternal empowerment in particular, are factors which can significantly influence the health of children and a child’s access to immunization. Two recent studies have examined this relationship between child health and overall gender equity at the national level. In a 2015 study looking at the degree of gender inequality among 138 countries with data from the United Nations Development Program, greater inequality between women and men was significantly correlated with a country having higher under-5 mortality rates and lower immunization rates. A second study found that among 45 low- and lower-middle income countries supported by Gavi, countries with the least gender equality (as measured by reproductive health, women-held parliamentary seats, educational attainment and other factors) also had lower vaccine coverage rates overall.
There are many ways in which a woman’s empowerment affects the health of her children. A child’s health – including the likelihood that they will be immunizated – in turn benefits from programs and policies that empower and educate women.
Educating women means children are more likely to get vaccinated
Studies have shown that maternal education is significantly associated with children’s immunization coverage. Researchers looking at vaccination coverage in 45 low- and middle-income countries found that children of the least educated mothers are 55% less likely to have received measles-containing vaccine and three doses of DTP vaccine compared to children of the most educated mothers. Another study looking at WHO data from member states shows that globally, coverage of the third dose of DTP is 26% higher among children born to mothers with some secondary education compared to mothers with no education. The increased likelihood of timely vaccination likely plays a role in the improved chances of child survival that are also associated with maternal education. An analysis conducted by UNICEF in 2015 found that across many South Asian and sub-Saharan African countries, children with mothers who received no formal education were almost 3 times more likely to die before reaching age 5 than those born to mothers with some secondary education.
The influence of empowerment and agency
Education is one important component or ‘resource’ that can empower women, but another key factor is a woman’s agency – her ability to define, and take action towards, personal goals. The degree of agency a woman may have is mediated by factors such as power over decision-making, access to money, social status, and freedom of movement. A 2016 systematic review of studies covering forty years of data from primarily African and Southeast Asian countries, found a trend where higher levels of women’s agency were linked to higher likelihood of complete immunization for their children. In another systematic review, in which qualitative research from low- and middle-income countries was analyzed to understand gender-related reasons for low vaccination rates, women’s low social status was shown to be a barrier to accessing vaccinations for their children. Specifically, key drivers of likelihood of vaccination included maternal education, family income, as well as a woman’s ability to control resource allocation and autonomous decision-making related to how her time is used.
One explanation for this effect may be that as agency increases, a woman may have more decision-making power to choose how household resources such as money and time are allocated; and if given the means, women often prioritize children’s health. In effect, her children’s good health is the goal towards which she will apply available family resources, to the degree her level of agency and resources allow.
Enticing evidence from one study indicates that empowerment and its positive benefits can be contagious. In a study of the impact on child immunization rates of a women’s empowerment program conducted among socially and economically disadvantaged women in India, it was noted that not only were the children of the women who had direct participation in the program immunized, but there was a measurable spill-over effect of vaccination to non-participants in program villages. Non-participating children in villages where the program occurred were anywhere from 9 to 32% more likely to be immunized against measles than children in villages without the empowerment program.
What can progress toward gender equity look like?
Sustainable Development Goal (SDG) 5
The Sustainable Development Goal (SDG) 5—to achieve gender equality and empower all women and girls—is a goal that is inextricably linked with progress on many fronts, particularly in the arena of women and children’s health. Similarly, the achievement of SDG 3 – to ensure healthy lives and promote wellbeing for all at all ages – rests on many factors, but both immunization and a concerted focus on gender disparities in low-income countries will be absolutely essential to this goal.
This focused approach on inequity makes both practical and financial sense. A 2010 study from UNICEF concluded that an equity-focused strategy would hasten progress towards health goals and be cost-effective, especially in low-income, high-mortality countries.2 Specifically, investment in a package of interventions designed to increase health equity, including access to immunization, was estimated to improve child mortality reductions by more than 20% over the status quo. Focusing programmatic efforts and supportive policies on the poorest or worst off in a population yields the greatest positive change with limited resources. Equity analyses can aid decision-makers in understanding both who is left behind or left out of progress on health and social fronts, and why.
Strategies which specifically target the health of women and children in an integrated way across interventions may be able to reverse gender inequity in immunization in some contexts. The National Rural Health Mission in Haryana, India, for example, implemented a multi-strategy community intervention program intended to reduce maternal and child health inequalities by improving healthcare at the household level in villages. Through the use of local incentives including cash, payment of travel costs, free hospital services for pregnant women, hospital-based treatment of neonatal illnesses, and locally appointed Health Activists, the program was able to eliminate gender inequalities for full immunization between male and female children. While such synergy between immunization visits and essential health care can be more involved to implement programmatically, the collateral gains make it worth pursuing in the service of creating healthier, more equitable societies.
Although much work has been done to identify child and family dynamics that underpin gender inequalities, more research and attention is needed to create change at the local and regional levels. Tailored strategies will be necessary in each setting to improve women’s agency and eliminate differential vaccination coverage for girls. Concentrating resources to improve gender equity in access to health will be integral to attaining global immunization and child survival goals, and can reinforce efforts to empower women worldwide.
For Additional Information:
1Alkema L, Chao F, et al. National, regional, and global sex ratios of infant, child, and under-5 mortality and identification of countries with outlying ratios: a systematic assessment. Lancet Global Health 2014; 2: e521-530.
2UNICEF. Narrowing the gaps to meet the goals, UNICEF, New York, September 2010.
In February 2018, Angela Chang and colleagues released a widely publicized study in Health Affairs estimating the death and economic impoverishment (due to medical expenses) that could be averted in 41 low-income nations through the use of 10 vaccine antigens from 2016-2030. Here, the VoICE team brings you “New Research Cliff Notes”, where we provide a high-level explanation of this new study, important considerations, notes on interpretation and drivers of the study’s estimates.
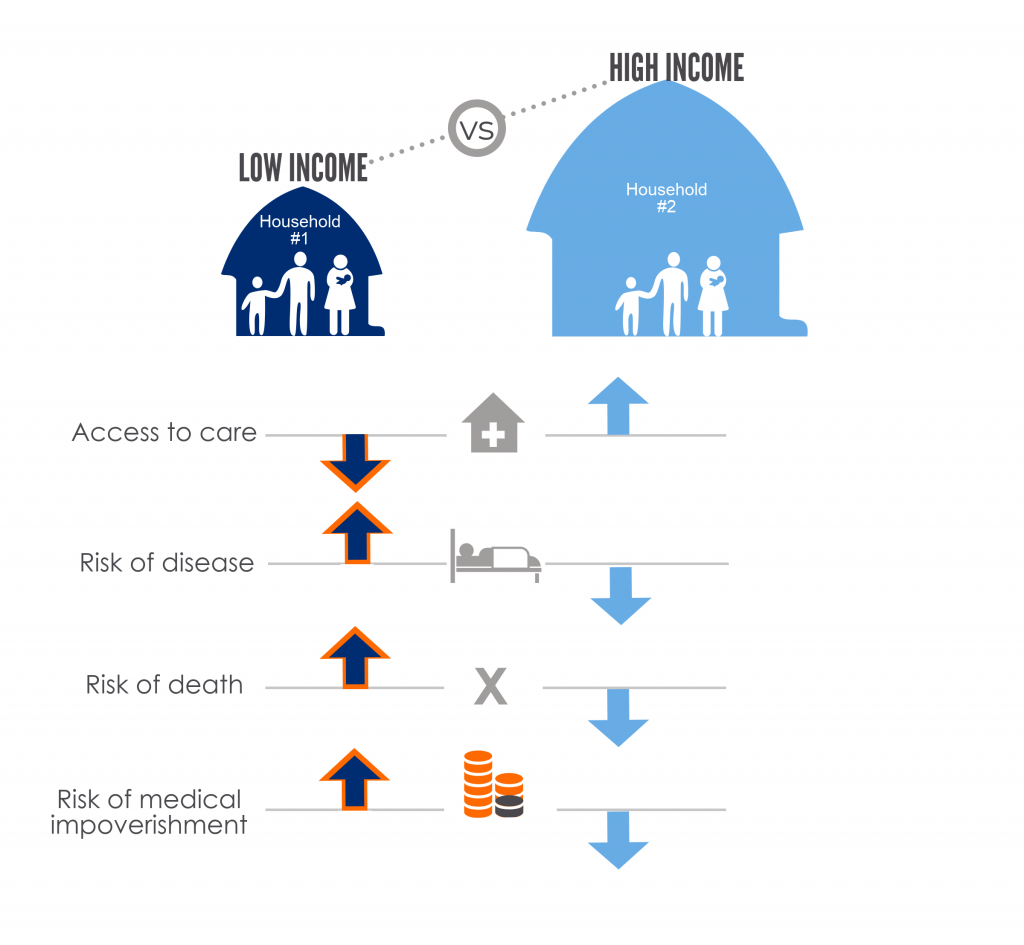
A pernicious cycle of poverty and ill health exist and vaccines can help to break this cycle. By preventing disease, vaccination also prevents the costs associated with disease treatment and thus helps to reduce the likelihood that households will fall into or remain in poverty. Within countries, greater benefits are observed among the poorest populations who often have higher risks of disease and death, reduced access to care, and are at significantly greater financial risk from medical expenses incurred to treat an episode of illness, as illustrated in Figure 1.
Figure 1: Drivers of health inequity and financial risk in low- vs high-income households
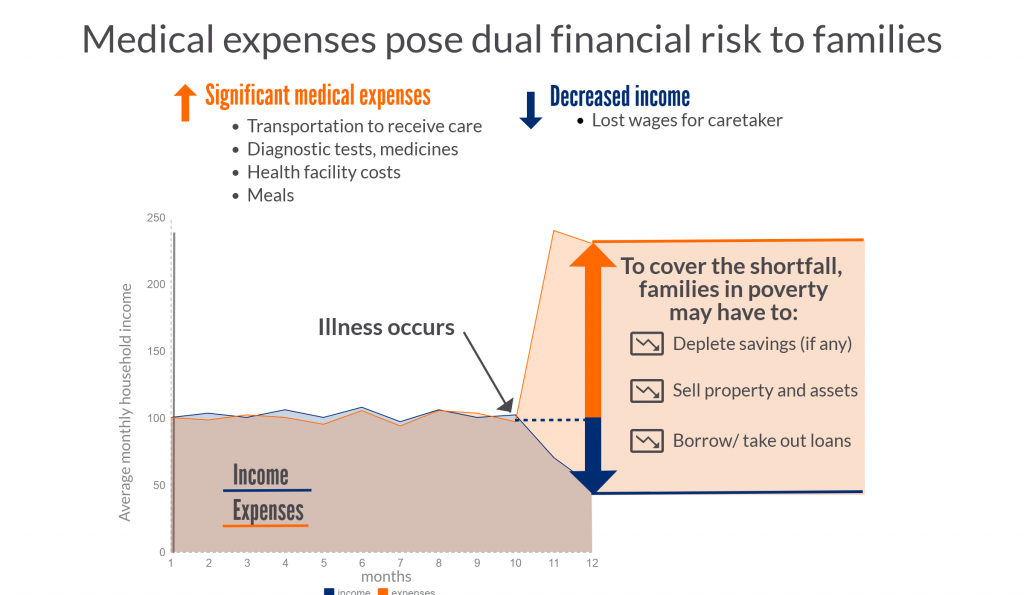
When children or adults become ill, families may have to use savings, sell property, or even take out loans to pay for their care. Additionally, their time spent away from domestic or paid work may impact negatively on their income. In short, an episode of illness can both increase expenses and reduce incoming finances, and thereby drive families into poverty. Figure 2 illustrates what can happen to a family living “paycheck-to-paycheck”, with limited or no savings and whose necessary expenses are roughly equivalent to their income.
Figure 2: The financial risk of unexpected medical expenses to a family living close to the poverty line
To what extent could vaccines impact this paradigm by preventing disease episodes leading to medical impoverishment? Recently, Angela Chang and fellow researchers have tried to estimate this, as well as to predict which people in low-income countries would reap the greatest health equity benefit and financial risk protection from vaccines. [Ref: Chang, et al. Health Affairs 2018]
The study: a look at the equity and poverty impact of vaccines
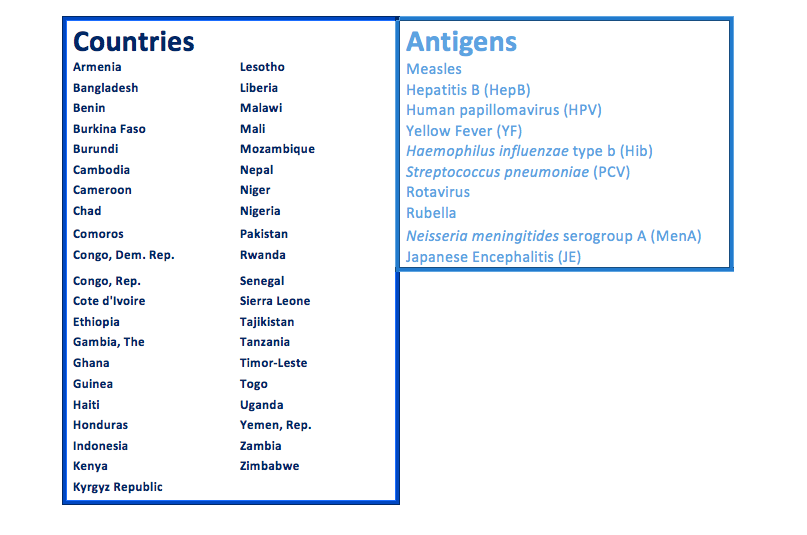
Chang and colleagues looked at the impact of 10 vaccine antigens in 41 low- and middle-income countries over the 15-year period of 2016 to 2030. (See Table 1 below) Using models to quantify the distribution of cases and deaths, the researchers compared the impact of these 10 antigens at expected coverage and efficacy levels, versus no vaccination. In this way, the authors could identify which vaccines should provide the largest benefits in terms of health gains, protection against financial risk, and equity.
Table 1: 41 countries and 10 antigens included in the equity and medical impoverishment analysis
What does it mean to have modeled data?
Models are mathematical equations that try to predict certain specified outputs that are difficult to empirically study based on inputted numbers. For example, you can estimate the number of disease cases in a population by using the incidence rate (that may be derived from a study in another population), and multiplying that by the number of people at risk of getting the disease in the population of interest.
Number of disease cases = new cases of disease per 100,000 persons x number of susceptible persons
Sometimes the inputs into a model are well-known, and sometimes there is a lot of uncertainty in the inputs used. In the latter case, that also means that the outputs of the models can vary a lot based on the model assumptions. For this reason, researchers should explain what assumptions they made to choose the inputs for their model. Often, modelers may also test different input values to see how variable the resulting estimates can be; this is called a sensitivity analysis.
Study findings: key drivers of the model
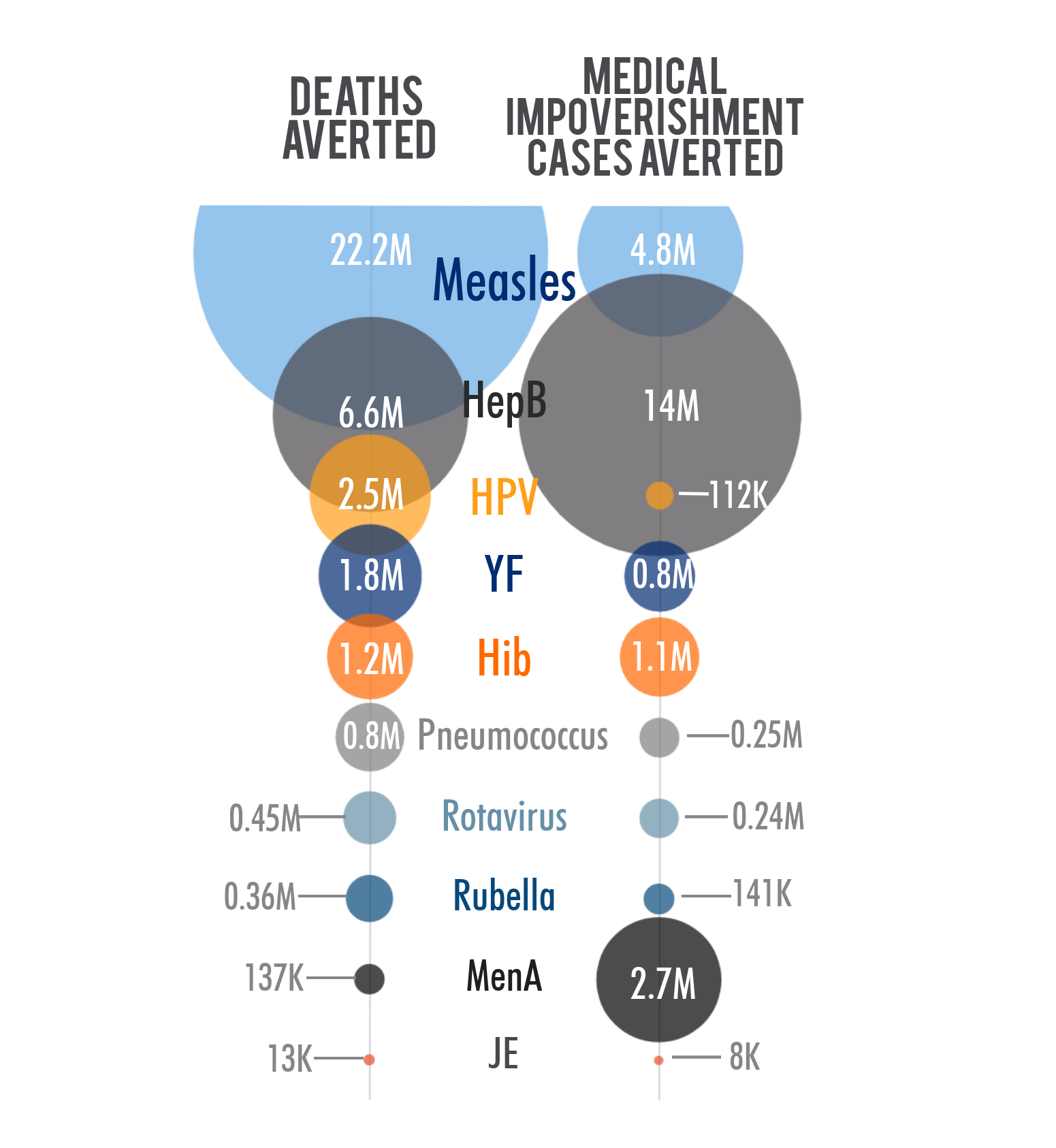
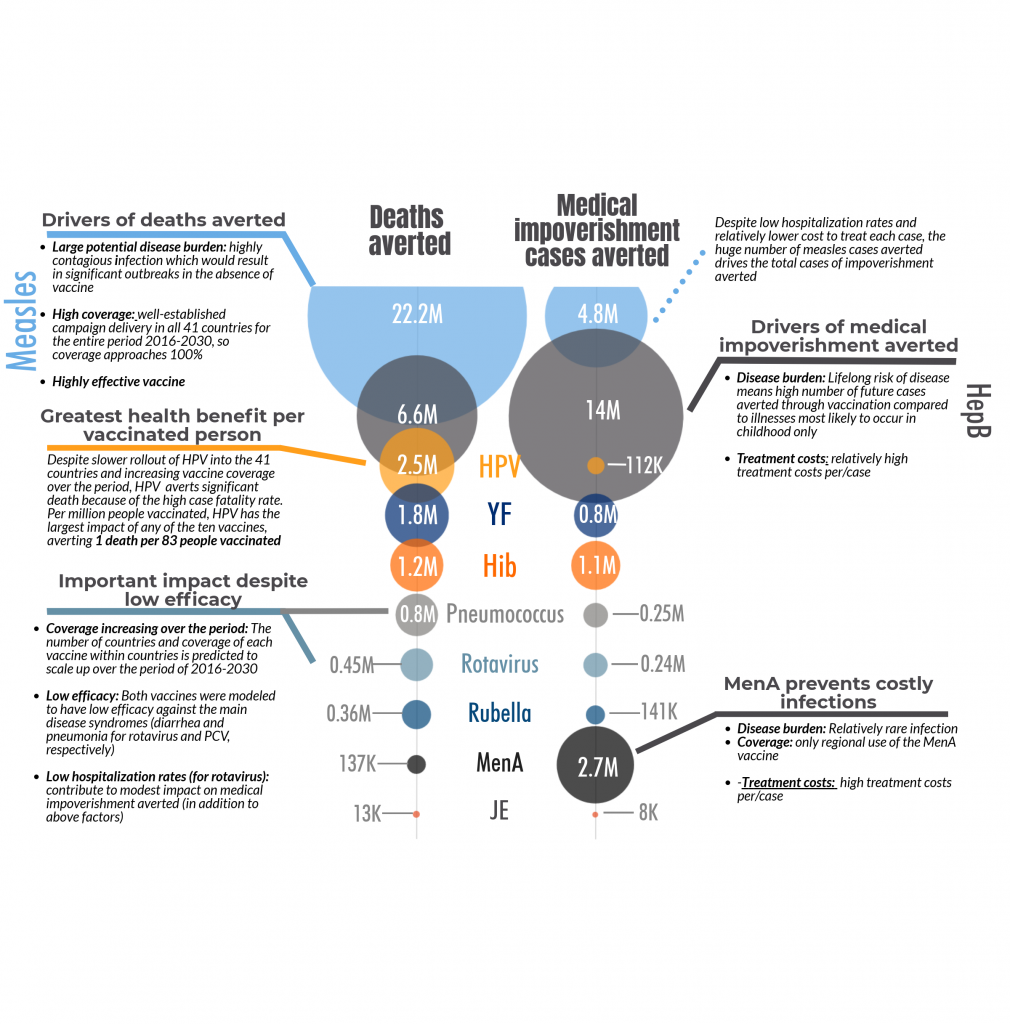
The model developed by Chang et al estimates that thirty-six million future deaths could be prevented by using the 10 vaccines during the period 2016-2030, compared to not using any of the vaccines. Measles accounted for 22 million deaths prevented, about 60% of the total deaths averted. There are several reasons why measles makes up such a large part of the mortality and medical impoverishment benefits, including: high, widespread coverage; measles infection is highly contagious and, in the absence of vaccination, would lead to significant outbreaks; measles has a relatively high mortality rate. (See Figure 3 below)
Medical impoverishment refers to the number of households that would be pushed below the poverty level due to the costs incurred from seeking, and paying for, treatment for a disease. The household poverty line was set at the World Bank level of $1.90 per day (2011 international dollars). Using these vaccines, researchers estimate that 24 million households that received immunizations between 2016-2030 would avoid falling below the poverty line. Hepatitis B and measles together account for about 80% of these cases.
It is important to note that in this study, those households that are already below the poverty line do not count towards the cases of medical impoverishment averted. However, these families would be further set back financially if they need to pay for medical care and would benefit significantly from the financial risk protection that immunization affords. That stark reality is that it is not uncommon for these families to make the hard decision not to seek care because they cannot afford to do so.
Figure 3: Drivers of deaths and cases of medical impoverishment averted through the use of 10 antigens in 41 countries, 2016-2030
As you can see from the notes in Figure 3, certain key input variables drive the results. However, two antigens may have similar impact estimates but for significantly different reasons. For deaths averted the key variables considered were:
Prevalence of risk factors for the disease by income level: for example, vitamin A deficiency or malnutrition, which are much more common in the poorest quintile than in the wealthiest
Number of countries using the vaccine between 2016 and 2030, and year of introduction
Expected vaccine coverage rate over time, in countries that have introduced a given vaccine
Effectiveness of the vaccine in preventing disease
Treatment coverage rate: how many people with the disease will seek medical care
Risk of death among cases of disease (case fatality risk, which includes a measure of treatment effectiveness)
Disease impact of vaccines: the poor have more to gain
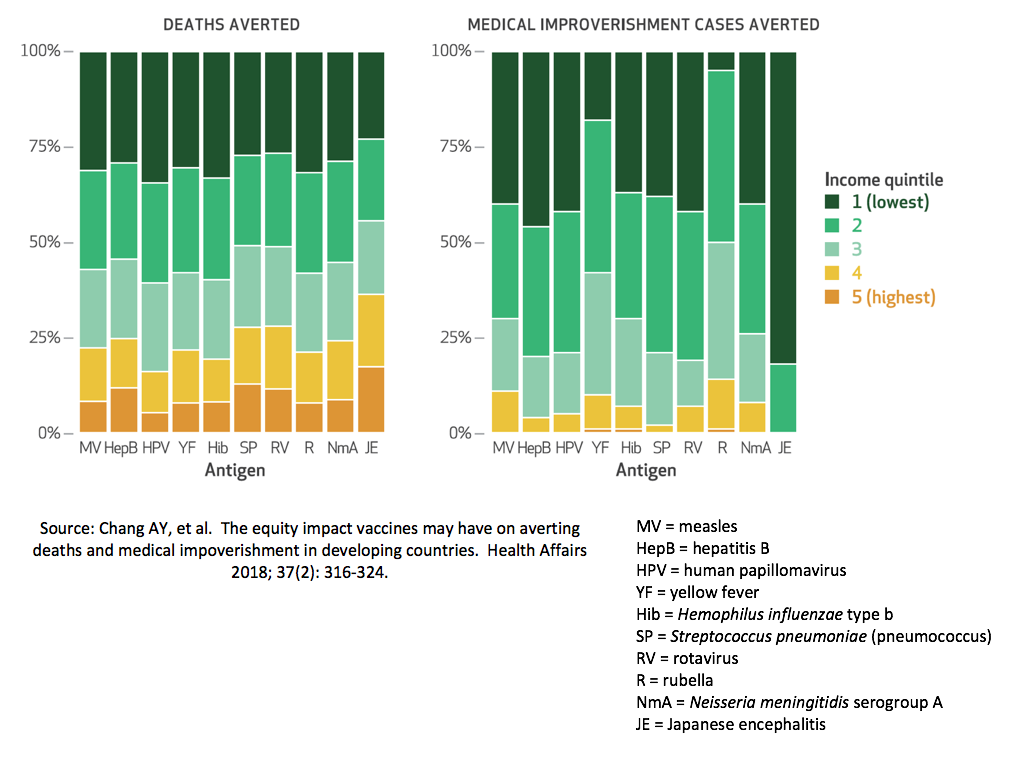
As seen in Figure 4 below, over half of all deaths averted for most diseases would come from those families in the lowest two wealth quintiles, the poorest 40% of households. People from these households are at higher risk of disease because they have a higher prevalence of risk factors (such as malnutrition or lack of sanitation) and poorer outcomes if they get sick. Also, because of the higher fertility rate, there are more people in the poorer income quintiles who are at risk of disease. So even though the poor have lower vaccine coverage rates in general, they have more to gain in terms of absolute numbers of averted deaths.
Illness-related poverty: who is at risk and what do the numbers mean?
For medical impoverishment, the most significant input variables for the model include:
The number of disease cases or burden of the disease
Care seeking behavior: how many people with the disease will seek medical care
Household financial risk (i.e. how close the household is to the poverty line before seeking disease treatment – See Figure 2 above for an example scenario)
Household expenses related to disease treatment, which can vary by:
Severity of illness
Length of hospital stay
Cost of hospital stay per day
Costs of tests and medications
Additional household expenses related to treatment including
Transportation costs to get to and from the clinic or hospital
The lost wages for time away from work because of medical care
Figures 3 and 4, above, illustrate some of the ways of considering what drives the numbers of illness-related poverty, and how the numbers predicted can vary based on the disease and vaccine context.
Important to note…
Those households that are already below the poverty line do not count towards the cases of medical impoverishment averted. The study evaluated how many people above the $1.90/day threshold would be pushed below that figure due to medical expenses, thus people already below the threshold are not counted. However, these already impoverished families would be pushed further into poverty if medical expenses were incurred, and would benefit significantly from the financial risk protection that immunization affords. That stark reality is that it is not uncommon for these families to make the hard decision not to seek care because they cannot afford to do so.
The equity and poverty reduction impact analysis can be measured in four dimensions:
burden of disease averted (e.g. deaths and cases of disease averted);
financial risk protection afforded by vaccines (i.e. the protective effect of vaccines against household expenditures for disease treatment)
transportation to health facility, productivity and wage losses
equity (distributional consequences among population subgroups (e.g. income groups, subnational regions); and costs needed to sustain the vaccine policy
Varying inputs to the model will also change the resulting estimates of deaths and medical impoverishment averted.
Some model inputs may affect the estimates for deaths and medical impoverishment cases differently. For example, higher healthcare utilization rates lead to a lower predicted number of deaths averted—because fewer disease cases progress to death when more people access care – but also result in higher predicted cases of illness-related poverty averted as more people would incur treatment costs when they access care.
Finally, a few key points…
Vaccination in low- and middle-income countries can substantially decrease child mortality but also prevent disease-related hospitalizations, health-related impoverishment, and bring significant financial risk protection to households.
Within countries, greater benefit is expected among the poorest populations who often have higher risks of death, reduced access to effective care, and bear significant economic costs due to disease treatment.
The total predicted number of cases of illness-related poverty averted—24 million—represents about 9% of people in low-income countries who are already impoverished. The use of these 10 vaccines prevents adding to the ranks of poverty by reducing disease burden and the associated—sometimes catastrophic—cost of care.
Care should be taken in comparing the relative benefits of different vaccines/antigens because the context for each significantly influences the broader impact on health and financial risk.
Each of the 10 vaccines evaluated had the greatest impact on deaths and medical impoverishment in the poorest 40% of households across these 41 countries.
Undernutrition and infectious diseases are tightly linked in a self-reinforcing cycle. Childhood episodes of diarrhea, pneumonia and measles are exacerbated by undernutrition, which significantly contributes to the death toll from these infections. In this feature, the VoICE team explains the cycle of malnutrition and infectious disease, and brings you evidence of the ways in which vaccines interrupt this cycle and help to protect the overall health, growth and physical development of vulnerable children.
A hidden killer: poor nutrition underlies almost half of all deaths in children under 5
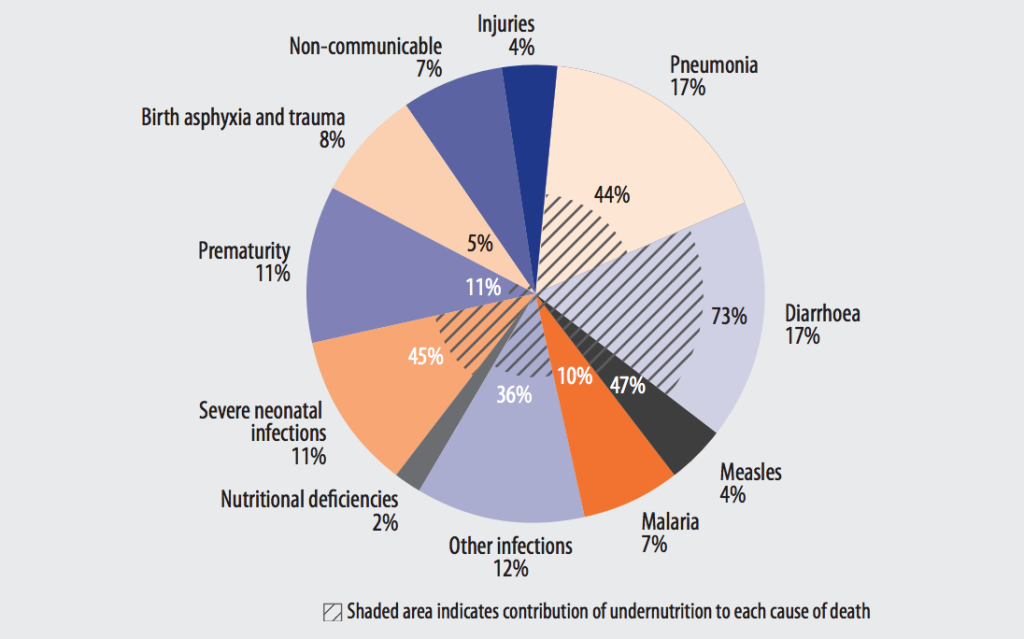
You won’t see nutrition listed as the cause of death in a pie chart of child mortality, but undernutrition is one of the key contributing factors behind child deaths due to infection. Undernutrition is defined as insufficient food intake—including calories and/or nutrients–to sustain growth and health. (Malnutrition, in contrast, is a broader term referring to both undernutrition and overnutrition—the excess intake of food and calories.) The WHO estimates that undernutrition is a factor in 45% of child deaths—contributing to over 3 million deaths in 2004 – including 73% of child deaths due to diarrhea, 44% of pneumonia deaths, 47% of measles deaths, and 45% of deaths due to severe neonatal infections (Figure 1).1, 2, 3 These are the top childhood killers, and they share a recurring theme: undernourished children get sick more often and have worse outcomes—including a higher risk of dying—from every episode of infectious disease.4
Figure 1: Major causes of death in children under 5 years old with disease-specific contribution of undernutrition, 20041
Source: WHO. Global health risks: mortality and burden of disease attributable to selected major risks. 2009. Click here for full report.
Many children worldwide are still undernourished
Undernutrition is common among children under 5, particularly in the poorest regions of the world, such as South Asia and Sub-Saharan Africa where 1 in every 3 children is undernourished. 5Undernutrition manifests in different ways as stunting, wasting and specific nutritional deficiencies of key vitamins and minerals that children need to grow and develop properly.
Stunting, as defined by a recent report from the WHO, UNICEF and the World Bank, refers to a child who is too short for their age.5 It is a result of chronic or recurrent undernutrition and affects 23% of children globally, or 155 million. Three-quarters of stunted children live in Sub-Saharan Africa and South Asia, where the prevalence of childhood stunting exceeds 33%. A more acute form of undernutrition is wasting, which refers to a child who is too thin for their height. Wasting results from rapid weight loss or a failure to gain weight and affects about 8% of children, or 52 million, under 5 globally. However, in South Asia levels are particularly critical with over 15% of children under 5 experiencing wasting.5 Notably, stunting is more prevalent than wasting as it is cumulative after multiple, shorter episodes of wasting—which in and of themselves can be reversible—but over time leads to stunting which is largely irreversible and has lifelong consequences.6
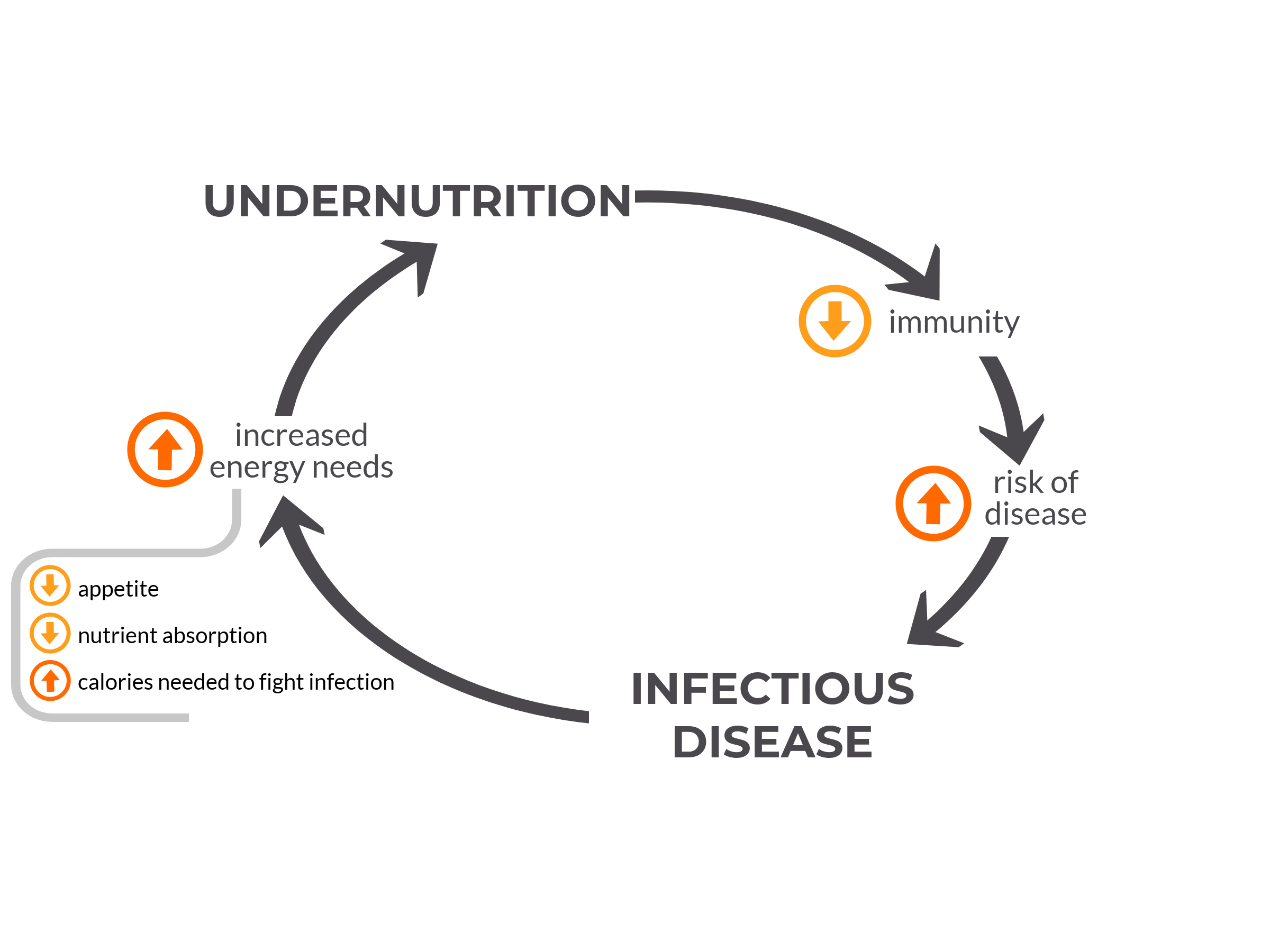
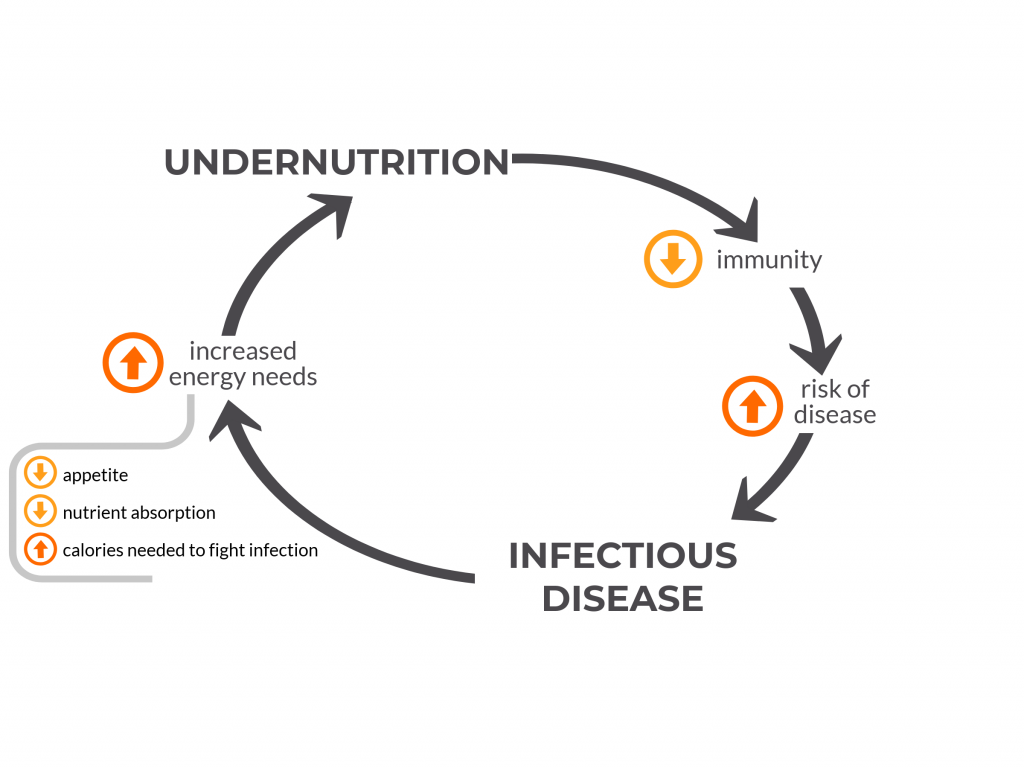
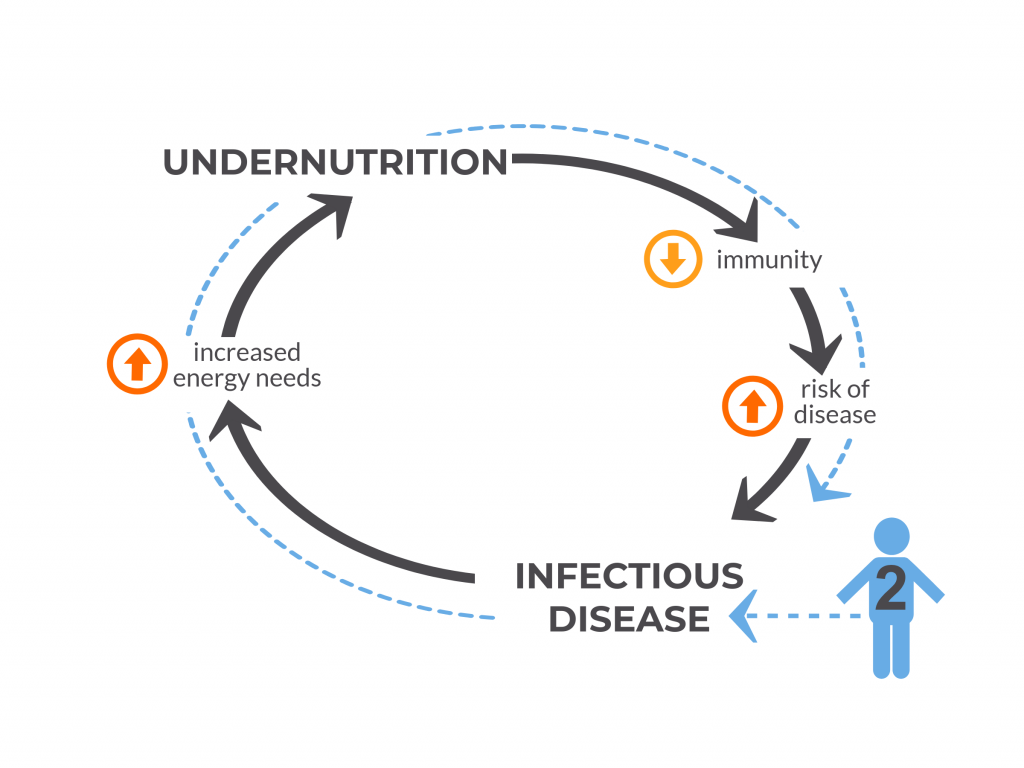
A vicious cycle: undernutrition and infection
Figure 2: The vicious cycle of undernutrition and infectious disease
Undernourished children have less nutritional reserves to grow properly and to fight off infections.
Undernutrition has been called the most common cause of immunodeficiency worldwide.7 With poor nutrition, some parts of a child’s immune system do not function properly. The skin and gut cannot effectively block disease-causing bacteria, viruses and parasites from entering the body. The thymus, a gland in the neck which helps develop the disease-fighting T cells, becomes smaller and other parts of the immune system do not function properly. Thereby undernourished children are put at increased risk of developing diseases to which they are exposed in their environment and against which they otherwise would normally be able to defend themselves.
With each episode of disease, some of the energy and calories a child would otherwise use for growth and development is diverted to fight off the infection. Calories are consumed to mount a fever, one of the body’s protective mechanisms. If the child has pneumonia, breathing requires more work and this will require more calories, too. If the child has diarrhea, less nutrients are absorbed while the gut is inflamed and infected. For these reasons, a sick child needs more energy and calories to fight off the infection and recover, and an undernourished child – who has fewer energy reserves and likely less access to nutrient-rich food to begin with – falls even further behind in fulfilling their nutritional needs and is more susceptible to the next bout of illness.8
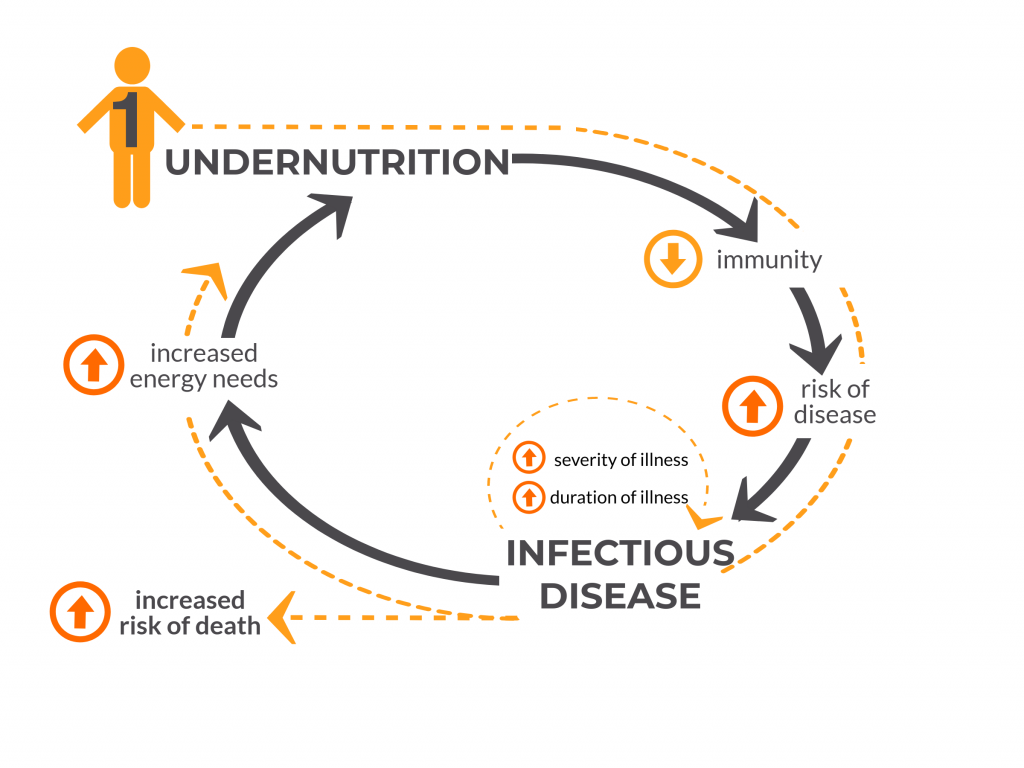
Figure 3: Child #1 is Undernourished
This decreases their immune system function, increases disease risk, duration and severity and significantly increases the risk of death. Infections further negatively impact nutritional status, potentially increasing the severity of undernutrition in this child and pushing them around the vicious circle once more.
A child who is sick also may not eat as much, taking in fewer calories and nutrients for the duration of the illness, putting the child at risk for falling further behind in growth. A prospective case-control study conducted in several developing countries found that children with moderate-to-severe diarrhea grew significantly less in length in the two months following their episode compared to age- and gender-matched controls.
Not only are undernourished children – like child #1 in Figure 3, above – more susceptible to getting sick, but their disease course is more likely to be severe or even fatal. A study of Bangladeshi children found that severely undernourished children had a nearly eight-fold increased risk of death from diarrhea than those who were not severely undernourished. In the case of pneumonia, those who are undernourished are at a 15-times higher risk of death. In this way, undernutrition is a hidden co-killer, masked behind the number of deaths due to diarrhea, pneumonia and other infections such as measles and malaria.
An otherwise healthy child – like child #2 in Figure 4, below – can also become temporarily undernourished because of an infection such as pneumonia, due to the increased energy needs of the infection. This can put the child at increased risk of other infections until a healthy nutritional status is attained once again.
Figure 4: Child #2 was not undernourished, but became undernourished due to an episode of infection.
This may set them upon the path of recurrent infection and undernutrition.
Sickness and undernutrition have long-term consequences for children’s growth and development
Recurrent disease, severe disease and undernutrition interact to shape the trajectory of a child’s growth and cognitive development in the critical first 1000 days of life with long-term implications. Certain severe infections such as meningitis leave many children with long-term cognitive impairment and neurological sequelae. In a systematic literature review of studies from Africa, it was found that one quarter of children who survived pneumococcal or Hib meningitis—two vaccine-preventable causes of meningitis–had long-term neuropsychological deficits.
Stunting has been linked with lifelong consequences such as diminished cognitive development and decreased economic productivity for affected individuals.8 Studies have estimated that undernutrition decreases a nation’s economic growth by 8% or more due to the reduced potential of its people to study or work to their full potential.9
Vaccines are an important component of breaking the vicious cycle
The interactions of childhood diarrhea, pneumonia and malnutrition contribute to a vicious cycle of poor health and delayed growth and development. Immunization, as an effective measure to protect against some of the main diseases of childhood, can help to disrupt this cycle.
Pediatric vaccines recommended by the WHO and UNICEF have been proven safe and effective in reducing children’s risk of disease and death. Vaccines such as pneumococcal conjugate vaccine (PCV) and Hib conjugate vaccine target bacteria that cause pneumonia and meningitis. Live, attenuated rotavirus vaccines target the leading cause of severe, dehydrating diarrhea in young children.11
Even children who are undernourished can respond well to vaccines, though there may be some differences in the amount or type of immunity they can produce depending on the degree of their undernutrition.9 More up-to-date studies are needed on the immune effects of undernutrition as much of the data on this topic is from older studies and using older laboratory tests. However, vaccines given to children on a timely basis have significant benefits for malnourished children and are integral in a multifaceted approach to breaking the vicious cycle of undernutrition and disease. In addition, many vaccines trials have been conducted in populations with high rates of stunting and wasting and have proven that even in these settings vaccines are effective and highly impactful.12, 13, 14, 15
These collateral gains of implementing a vaccine program were also observed in an Indonesian study of 24 communities, which found that children living in communities with higher overall levels of immunization were less likely to be malnourished as measured by how thin they were for their age.
According to a WHO report on global health risks, vaccines are part of a multi-pronged approach to reduce childhood underweight (along with nutritional interventions – such as micronutrient supplementation for children and women of child bearing age, and exclusive breastfeeding in infancy), which is the leading risk factor for death and disability in low income countries.1 By protecting children against common and sometimes deadly diseases, vaccines play a role in breaking the vicious cycle of infection and turning the tide on the hidden epidemic of undernutrition.
FOR ADDITIONAL INFORMATION:
1WHO. Global health risks: mortality and burden of disease attributable to selected major risks. 2009. Available at: http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf. 2Bhutta ZA, et al. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet 2013; 382: 452-477. 3RE Black, CG Victora, SP Walker, et al., the Maternal and Child Nutrition Study Group. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet (2013) published online June 6. 4WHO Media centre. Children: reducing mortality. 2017. http://www.who.int/mediacentre/factsheets/fs178/en/ 5UNICEF, WHO, World Bank. Levels and trends in child malnutrition: UNICEF/ WHO/ World Bank Group joint child malnutrition estimates, key findings of the 2017 edition. 2017. Available at: http://www.who.int/nutgrowthdb/jme_brochoure2017.pdf?ua=1. 6WHO. Stunting. Accessed at http://www.who.int/mediacentre/infographic/nutrition/infographic-stunting.pdf?ua=1. 7Prendergast AJ. Malnutrition and vaccination in developing countries. Phil Trans R Soc B 2015; 370: 20140141. 8Katona P and Katona-Apte J. The interaction between nutrition and infection. CID 2008; 46(10): 1582-1588. 9S Horton, RH Steckel Global economic losses attributable to malnutrition 1990–2000 and projections to 2050. B Lombard (Ed.), appearing in: How much have global problems cost the world? A scorecard from 1900 to 2050, Cambridge University Press, Cambridge (2013)
10Black RE and the Maternal and Child Nutrition Study Group. Maternal and child nutrition: building momentum for impact. Lancet 2013; 382: 372-375. 11WHO. Rotavirus vaccines: WHO position paper—January 2013. WER 2013; 5(88); 49-64. 12Isanaka S, et al. Efficacy of a low-cost, heat-stable oral rotavirus vaccine in Niger. NEJM 2017; 376: 1121-1130. 13Cutts FT, et al. Efficacy of nine-valent pneumococcal conjugate vaccine against pneumonia and invasive pneumococcal disease in The Gambia: a randomised, double-blind, placebo-controlled trial. Lancet. 2005;365:1139-46. 14Madhi SA, et al. Effect of human rotavirus vaccine on severe diarrhea in African infants. NEJM 2010; 362(4): 289-298. 15Watt JP, et al. Haemophilus influenza type b conjugate vaccine: review of observational data on long term vaccine impact to inform recommendations for vaccine schedules. 2012. Available at: http://www.who.int/immunization/sage/meetings/2012/november/5_Review_observational_data_long_term_vaccine_impact_recommendations_vaccine_schedules_Watt_J_et_al_2012.pdf.
Childhood pneumonia is arguably the most unfair affliction in the world. Not only is pneumonia the leading infectious cause of death in children less than 5 years of age – taking the lives of more than 100 children each hour, nearly a million per year – but it disproportionately affects those living in the poorest households and in the poorest countries around the world. Hib, pneumococcal, measles and pertussis vaccines are turning the tide in the battle against childhood pneumonia, and are helping to erase the complex inequity into which children living in poverty are born. Read on to find out why and what role vaccines are playing in the war on poverty.
A description of the hardships associated with everyday life for children in poor households reads like a top ten list of risk factors for childhood pneumonia and pneumonia mortality. Common issues such as malnutrition, poor access to care, overcrowding, immune-compromising infections, low levels of parental education and more all contribute to the stark fact that a child born in the poorest fraction of society has many times the risk of pneumonia and death compared to a child born in the wealthiest fraction. Here we provide some of the most important ways in which poverty-associated factors impact a child’s risk of pneumonia:
The vicious cycle of poverty-associated risks
Sick kids get sick more often, negatively impacting growth and development
Children whose immune systems are weakened by factors more common among the poor – such as diarrhea, measles or malnutrition – are at significantly increased risk of pneumonia, which in turn increases the risk of subsequent infections and inhibits healthy physical growth and development.
A recent review of data from developing countries found a negative feedback loop between pneumonia, diarrhea and malnutrition whereby suffering from of any one the three conditions increased a child’s risk for the other two.
Studies from Kenya to the Philippines to India have demonstrated how infections like pneumonia and diarrhea are linked to poor growth in childhood and can further impact an already weakened immune system
According to UNICEF, more than half of the children who die of pneumonia before their fifth birthday also suffer from undernutrition.
Weakened immune systems mean greater risk of pneumonia
Rates of HIV infection in children are highest in some of the world’s poorest countries, especially in Africa. HIV and other conditions, such as sickle cell disease, compromise a child’s ability to fight off infections and increase the risk of pneumonia and death.
HIV exponentially increases the risk of pneumonia and pneumococcal infections among both children and adults. Data from South Africa found that HIV-positive people had more than 40 times the risk of invasive pneumococcal disease borne by HIV-negative
Sickle cell disease, which affects nearly a quarter of a million African children born each year, increases the risk of Hib disease by more than 12-fold and the risk of pneumococcal disease by more than 35 fold, according to a 2010 review of bacterial infections in African children.
Breathing polluted air = more pneumonia
Kids regularly exposed to indoor and outdoor air pollution are at greater risk of developing pneumonia. Indoor pollution is common among poor households whose meals are prepared over solid fuel fires in the home or who use these fuels for heating.
A 2016 UNICEF Report noted that indoor air pollution contributed to more than 50% of pneumonia
Poor kids, and those with less educated parents, are less likely to be immunized
The relationship between poverty and education is well-documented and both factors have a significant and negative impact on the likelihood of vaccination among young children.
A study from Uganda found that the children of mothers whose education continued past primary school were 50% more likely to have received scheduled vaccines than children of mothers with less education.
Data from WHO member states was analyzed by researchers who found that children born to mothers with some secondary education were over 25% more likely to have received the third dose of DTP than mothers with no education. (Note: Coverage with the third dose of DTP3 is the most commonly used indicator of routine immunization coverage and program strength.)
A review of immunization coverage in India found that household wealth was directly correlated with the likelihood of immunization. Greater parental education also increased the likelihood of immunization.
Children living in slums have significantly lower vaccination rates than other children. A review of the health of kids in slums noted that vaccination rates among kids in slums in Niger were less than half that of other children.
The world’s poor will reap the most benefits from pneumonia vaccines
Given the significantly increased risk of pneumonia – and recurrent infections – borne by children in poverty, it stands to reason that these children will benefit the most from the protective boost afforded through vaccines such as Hib, pneumococcal and measles vaccines. By directly preventing infection with these common causes of severe pneumonia, vaccination against these diseases protects a child’s underlying health status – which in turn protects against other illnesses such as diarrhea – and facilitates healthy growth and development overall. The economic benefits of these vaccines for poor families and low-income nations are significant and will play a key role in meeting the Sustainable Development Goals.
Pneumonia vaccines help interrupt the vicious cycle of childhood infections and improve growth
A review of malnutrition and childhood infections in developing countries concluded not only that pneumococcal vaccine helps protect a child against subsequent illnesses like diarrhea but also measurably improves a child’s growth (height and weight).
Vaccines protect the most vulnerable and the unvaccinated
A large randomized controlled trial of a pneumococcal conjugate vaccine in South Africa found that use of the vaccine prevented 10 times as many cases of pneumococcal pneumonia in HIV-positive children than in HIV-negative children
Vaccines against pneumonia increase health AND wealth equity
Between 2016 and 2030, researchers estimate that the use of pneumococcal and Hib vaccines in 41 low- and middle-income countries between will avert more than 1.25 million cases of medical impoverishment, a phenomenon where families are pushed below the poverty line due to the costs associated with medical treatment for childhood infections. More than half of the two million deaths averted through the use of these vaccines would occur among the poorest 40% of the population of these 41 countries. (Stay tuned to the VoICE eBulletin in April for an in-depth feature on this new study!)
-A study in Ethiopia found that 30-40% of all deaths averted by introducing PCV would occur in children in the lowest wealth quintile, while also protecting the poorest families from exposure to financial hardship
The costs of treating illness can be significant for families with little or no savings. Families in Bangladesh are heavily borrowing money or selling whatever assets they may have to afford treatment for their children
Hib and Pneumococcal vaccines unlock a host of additional benefits
The Hib and pneumococcal bacteria are also important causes of meningitis, sepsis, ear infections and more. Protecting children from Hib and pneumococcal pneumonia thus carries the added benefits of protecting against these additional infections which themselves carry significant economic, health and cognitive costs. Stay tuned to future editions of the VoICE eBulletin to find out more about the benefits of Hib and pneumococcal vaccines, including:
Protection against life-threatening meningitis and sepsis
Tempering the threat of antibiotic resistance and overuse
Leveraging the theme of World Immunization Week (April 24-30), Protected Together #Vaccineswork, the VoICE team has developed social media content pairing evidence from the compendium with the priority messaging areas of WIW2018 advocacy partners. We invite you to download our WIW2018 social media toolkit.
Evidence from several disciplines indicates that immunization has a broader role to play in lessening the impact of cancer than one might expect. While it may be obvious that the widespread and growing use of vaccines against Hepatitis B and human papilloma virus (HPV) is directly responsible for preventing a significant number of related cancers, immunization against a host of other diseases may indirectly help to prevent additional cancers while helping to protect the health of immune-compromised cancer patients considerably. Read on for a brief explanation of how vaccines can prevent cancer, protect cancer patients and more.
The direct benefits of preventing cancer-causing infections
HepB and liver cancer
Introduced in 1982, the hepatitis B vaccine was the first widely available vaccine to directly prevent cancer. More than 1 billion doses of HepB vaccine have been delivered, resulting in a significant reduction in the chronic liver infection that leads to cirrhosis or cancer in roughly a quarter of adults. The risk of HepB infection begins at birth – and lasts throughout a person’s life – which is why HepB is the first vaccine most children receive, often within hours of coming in to the world. In fact, 80-90% of children who are infected with HepB during the first year of life will go on to develop chronic liver disease, dramatically increasing their cancer risk.
A leading cause of death among women, cervical cancer took the lives of more than a quarter of a million women in 2012, 85% of whom were from low- or middle-income countries. Cervical cancer is caused by human papillomavirus (HPV), a common infection that can lead to abnormal cell growth and high-mortality cancers. Just two of the more than 100 strains of HPV are responsible for 70% of cervical cancers and precancerous lesions. Each of the three available HPV vaccines has been proven effective in preventing infection with high-risk strains of HPV and could protect against other forms of cancer caused by the virus. The exceedingly high mortality rate for cervical cancer (1 in 2 women will succumb to the disease) is due largely to the lack of access to early detection and treatment for women in much of the world, and reinforces the urgency of prevention through vaccination.
Some intriguing new evidence suggests that vaccines against HepB, Hib and polio may indirectly help to prevent the development of childhood cancers. Some scientists have suggested that early and robust stimulation of a child’s immune system – such as that afforded by vaccination – could help the body recognize and neutralize early tumors, thus decreasing the risk of developing certain childhood cancers such as leukemia. A study from the state of Texas in the US tested this idea and found that children born in counties with high coverage of HepB, polio and Hib vaccine were 33-42% less likely to develop a specific kind of leukemia than children born in counties with low vaccine coverage. Although only a small number of studies have demonstrated this indirect benefit of immunization on childhood cancers thus far, it is an exciting new area we will be following closely.
Protecting cancer patients and survivors from other infections
Cancer and cancer treatments can severely diminish the body’s capacity to fight infection, putting cancer patients and survivors at significantly greater risk of vaccine-preventable diseases and death from secondary infections. For example, a study of adults in the US found that invasive pneumococcal disease was more than 20 times more likely to occur in cancer patients than in cancer-naïve people. In a large study that followed survivors of childhood and early adult cancers for more than 5 years, researchers found a significantly higher rate of infections than in the siblings of these patients. Cancer survivors in this study were also 4 times more likely to die of infectious causes than their siblings. Pneumonia, a potentially vaccine-preventable infection, carried some of the highest increased risk to cancer patients, even more than 5 years after cancer diagnosis.
Survivors of pediatric and young-adult cancers must also be concerned about developing other forms of cancer later in life, some of which may be preventable through use of the HPV vaccine. A large study in the US found that longterm cancer survivors – both men and women – appeared to have a significantly increased risk of developing HPV-associated cancers and malignancies later in life. For these reasons, it is critical that cancer patients and survivors be vaccinated, and sometimes re-vaccinated, to ensure the greatest possible protection from additional infection.
The economic benefits of cancer prevention are substantial
Preventing cancer has significant economic implications, and vaccines that help prevent cancer carry a significant return on investment in a variety of settings.
Hep B: Economic benefits
In terms of economic benefits, HepB vaccine carries a high economic return on investment, due in part to the sustained risk of infection across the lifespan. Health economists have estimated that during the decade 2011-2020, the use of this vaccine in the world’s poorest countries will have a return of over nine times its cost, thanks to the widespread use and high effectiveness of HepB Vaccine.
Despite gradual uptake of HPV vaccine among the world’s poorest countries, health economists have estimated a 3-fold return on investment from the use of HPV vaccine in these countries during this decade (2011-2020). Averting the premature death of women through prevention of cervical and other HPV-related cancers increases overall productivity and would prevent destabilization of families and communities.
[1] High vaccine coverage in the general population significantly reduces the chance that an infectious agent is transmitted to others, significantly reducing the risk that an unvaccinated person will be exposed and infected. This phenomenon is called herd immunity.